Sport Injuries in Karate Kyokushin Athletes
Background
Over the last several years the martial arts became an
increasingly popular activity and benefited people of all ages. They
can lower level of aggression, improve self-reliance, self-discipline
and improve physical body [1], for example: cardio-respiratory and
musculoskeletal systems, body composition [2,3]. Instead of positive
profits, each of martial art style has many risks such as accidents
and injuries. The risk of experience variable injuries is dependent
on a style (technical aspects of each style), hours of training and a
degree of competitiveness [1,4]. In karate style injuries are mostly
associated with the karate striking surfaces for both sides- hands
and feet and therefore they can be often damaged by attacking
and other body parts can be damaged because of receiving a hit.
In the past, karate competition was without any safety equipment.
Doctrine of kyokushin style was to be hard and tough, so there was
no protection equipment. In traditional form of kumite (karate
competition), attacks to the head were prohibited and punishable
even with disqualifications. Nowadays, to meet modern criteria of
combat sports, protection gear is used.
It differs to certain tournaments and mastery levels which
comes along with rank of a games. Allowance of protection also
changes traditional rules, so attacking to a head is allowed now. This
is crucial to quantitative analysis of the strikes, as head is mostly
accessible by roundhouse kick and other type of high kicks. Common
protection for such strikes is to protect head with forearms. But
in some cases, striking feet may accidentally hit the elbow, when
opponents try to protect himself, when kick trajectory is badly set.
Foots are also vulnerable while performing low kicks, as opponents
try to block with their shins and knees. Badly executed technique or
bad aiming may also lead to injury of attacker instead of delivering
damages to an opponent. In case of fists, hits also are blocked (still,
hitting a face with hands are prohibited in this style). Protecting
with forearms, especially elbows are may cause more damage to attacker
than for blocker. Moreover, successful, powerful strikes may
deliver severe damages to opponent when hits are constructive.
For that purpose, protection gear for hands, shin and foots,
head and teeth and suspensor are allowed. But their use is
not obligatory, and some of athletes tends to not use it as from
subjective feeling they affect a movement or simply they believe
that use of such equipment are not the way of this martial art. Usage
of such equipment differs among athletes. Central organs such head
or genitalia are more sensitive, and athletes are more prone to use
protection for that areas, but choice of distal parts protection varies.
Exact distribution of injuries with or without such equipment
through an athlete carrier is not fully studied yet. Moreover,
collision injury is one of possible type, but there are also injuries
that comes with overuse of body part as accumulated damages to
ligaments which may led to torsion or backpain. Strikes requires
lot of full body rotation, so there is considerable torque applied
to spine ligaments each times they strike. In bad circumstances,
when overload accumulates and because of counterforce of
opponent workload for back’s ligaments are to severe, it may
lead to an injury or in light circumstanced to lower back pain for
sometimes in case of only some torsion or microdamage. Finally,
the aim of this study was to analyze the injuries occurring in top
elite karate kyokushin athletes. From premises presented above,
which describes circumstances of injuries and possible severity of
damages, following hypothesis were formed:
a. Most of athletes are willing to use protection of central
parts (breast, suspensors).
b. Women athletes are more prone to use protective
equipment than male athletes.
c. Injuries were more frequent among distal part of a body
than central ones.
d. Males suffers more injuries than a woman.
4. Material and Methods
Questionnaire survey designed by the authors was conducted
amongst the group of 61 people participating in Kyokushin
Karate European Cup in 2015 and XLIV Polish Karate Kyokushin
Championships in 2017 selected randomly. The inclusion criteria
for the study were: regular participation in karate training, at least
three years of competition and consent to participate in the study.
Exclusion criteria were: lack of consent to participate in the study,
irregular participation in karate trainings and too short training
experience (less than three years of competition). Then the 61
athletes were divided into 2 groups. The first group consisted of
40 males and the second consisted of 21 females. The largest group
were athletes with black belts- 82% and brown belts 18%.
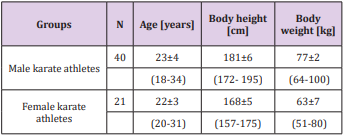
Among males, the mean age of was 23±4 years (18-34), mean
weight of 77±2 kg (64-100), mean body height of 181±6 cm (172-
195). 36 individuals showed right laterality of the upper and lower
limbs, ambidexterity was declared by 4 people. Among the male
group the mean of training experience was 10,8±3 years.
These athletes practiced karate approximately for 5 times per
week, additionally they practiced another kind of physical activity
for more than 3 times per week. Among females in turn, the mean
age of was 22±3 years (20-31), mean weight of was 63±7 kg (51-
80), mean body height of was 168±5 cm (157-175). 19 females
showed right laterality of the upper limbs, left one - remaining 2
females. Prevailing right laterality of the lower limbs (18 females),
while left and right laterality of the lower limbs declared 3 of them.
The mean of training experience was 11,8±3 years. These athletes
practiced karate approximately for 5 times per week. Also they
practiced other physical activities for almost 4 times per week.
Characteristics of the study groups are presented in Table 1.
The method of diagnostic survey questionnaire technique was
used. Karate athletes anonymously filled out the individual author’s
questionnaire, consisting of questions about: gender, age, height,
weight, laterality of the limbs, length of training experience, stage of
karate training, severity of the trainee, frequency of other exercises,
using protectors to avoid the injury, frequently recurring injuries,
how many times during training or competition a particular part
of the body was injured and about serious or permanent damage to
the respondent’s health [Appendix]. Survey results were collected
and subjected to statistical analysis using Microsoft Excel and
Statistica v.10 (StatSoft). The mean, standard deviation, minimum
and maximum values, Mann U Whitney test and severity rates of
specific indications were calculated.
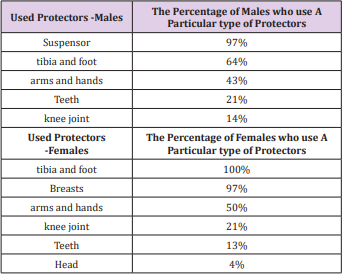
Karate athletes were asked to indicate what type of protectors
they use to prevent or minimize the risk of injury. In the first group,
the most common protector was suspensor (protector of the genitals), used by 97% of the karate practitioners. Other often used
protectors were leg - the tibia and feet (64%), upper extremities
and hands (43%). Several athletes have also used a teeth guard
(21%) and knees protector (14%). All questioned female athletes
to minimize the risk of injury applied at most tibia and foot protectors (100%), then -breasts protector (97%) , arms and hands
(50%), knee (21%) and teeth (13%). One of the women used additionally head protector. There was no person who did not use any
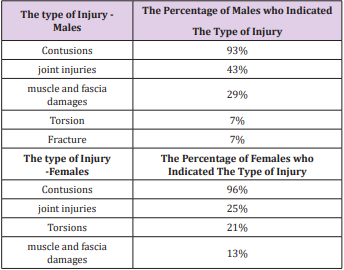
protection during exercises (Table 2). Karate athletes were asked to
indicate the most common injuries. In the study group prevailed:
contusions (91%), joint injuries (49%) with a total number of 548
different types of injuries, especially related to the left foot (23%)
and right hand (19%).
Athletes reported also selected cases of torsion (7%) and
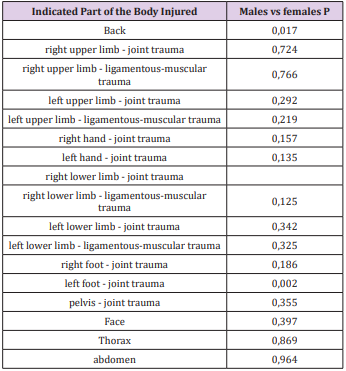
fracture (7%). There was not statistically significant difference in
the types of injuries between study groups except of injuries of
the left foot (p=0.002) and back (p=0.017). The results are shown
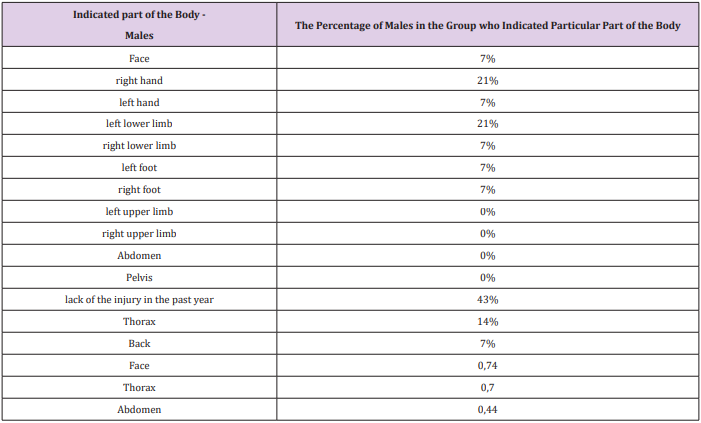
in Tables 3 & 4. Subsequently, contestants were asked to indicate
how many times during karate training particular part of the body
was damaged and were asked about injuries that occurred in the
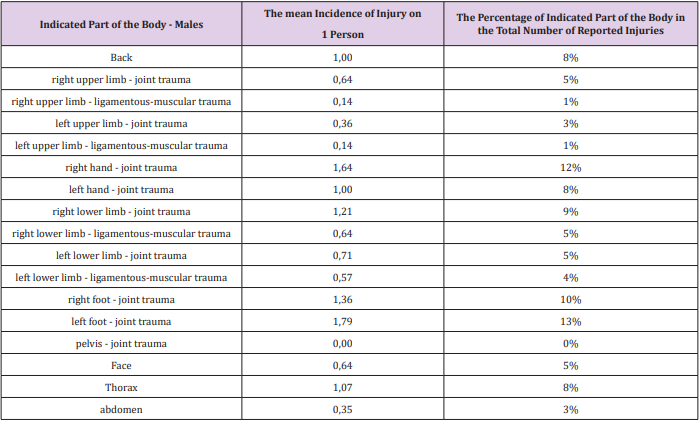
body during the last year. The results are presented in Tables 5-7.
In the first group most injuries were related to the left foot (13%),
right hand (12%) and right foot (10%). Reported cases of the right
lower extremity injuries (hip injury, 9%), chest, left hand, back (all
at 8%), right upper extremity (hip injury), face, right leg
(muscleligamentous injury), left leg lower (joint sprain) (all at 5%),
left
lower limb (ligamentous injury-muscular, 4%), left upper limb
(joint injury 3%) and abdominal (3%). Joint injuries were more
frequent than muscle damages. There was no report of pelvis injury.
There was no person who does not suffer any injury of the
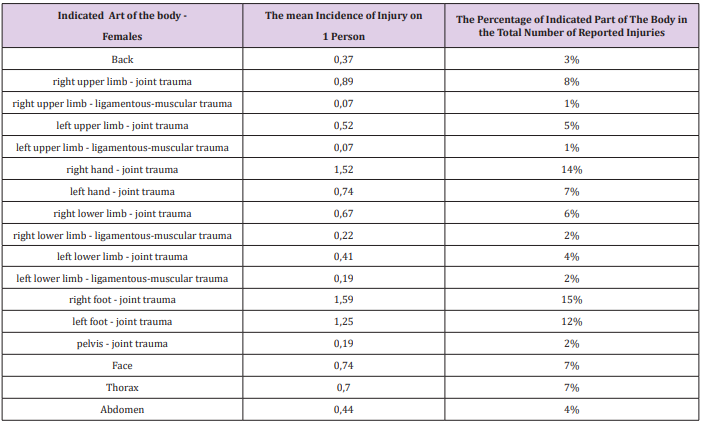
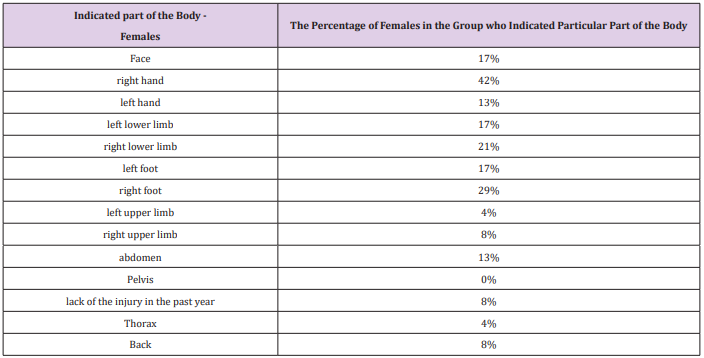
mentioned. The results are shown in Table 5. In the second
group, among women while practicing karate the most commonly
reported injuries were related to the: right foot (15%), right hand
(14%) and left foot (12%). Reported cases of right upper extremity
injury (injury to the joint 8%), left hand (7%), chest, face (7% each),
right arm (joint sprain, 6%), left upper extremity (hip injury 5%),
left lower limb (hip trauma - 4%), abdominal (4%), back (3%),
right left leg (ligamentous-muscular injury 2%), and left and right
upper limb (ligamentous-muscular injury 1%). Joint injuries were
more frequent than muscle ones. Responses are shown in Table 6.
Respondents suffered a total of 548 different types of injuries - 186
injuries among women and 362 injuries in men. Mean rate of injury
for one person among men were: 0.78, in which the right hand was:
1.64, left hand was: 1.0, right foot was: 1.36, left foot was: 1.79;
head
was: 0.64. For women, the mean rate of injury for one person was:
0.62, including the right hand: 1.52, left hand: 0.74, right foot: 1.59,
left foot: 1.25, head 0,74. In the past year in the group of males,
43% of them did not suffer injury. Most injuries underwent were
right hand (21%), left lower limb (21%) and chest (14%). Reported
isolate cases of injury to face, left hand, right leg, foot and back
(all
at 7%) (Table 7). In the second group, in the last year 8% of karate
kyokushin female athletes did not suffer any injury. Similarly, as in
male group, the most occurring was the right hand injury (42%).
Subsequently - right foot (29%), right lower limb (21%), face
(17%), left lower limb (17%), left foot (17%). There were several
cases of abdominal trauma (13%), left hand (13%), right arm (4%),
chest (4%) and back injury (8%). Responses are shown in Table 8.
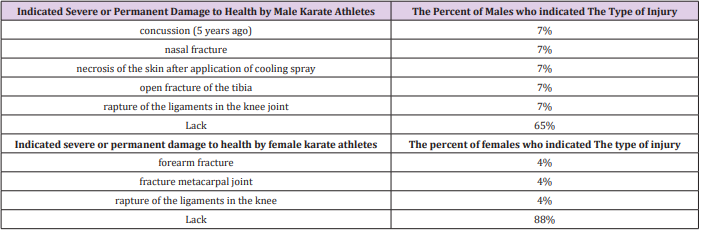
Lastly, athletes were questioned whether during training they
encountered with serious or permanent damage to the health.
Serious and permanent injury occurred rarely. In the first group
experienced them 35% of males and in the second group it was
12% of females. In the first group 65% of men during long-term
training were not encounter with a severe or permanent damage
to the health. The other karate athletes mentioned: bone fractures -
tibia and nose, a concussion (5 years ago), damage to the ligaments
of the knee joint and incompetent use of cooling spray resulting
in necrosis of the skin. In the same group, 88% of females have
no experienced serious or permanent injury. Other women from
the first group mentioned: fractures-of the forearm, metacarpal
bones and knee ligament damage. Respondents completing the
survey were asked to answer questions about the frequently
recurring injuries, how many times during training or competition
a particular part of the body was injured without their mechanism
of occurrence. The results are shown in Table 9.
Arriaza and Leyes [3] analyzed the injuries sustained by
athletes training karate: shotokan, shito-ryu, goju-ryu and wadoryu - taking part in three consecutive World Championships. The
mean value of the injuries was at level 157.03/1000 competitors.
Authors reported 891 injuries. The most common injuries were
contusions of the large muscle groups (50.3%), facial traumas
resulting in bleeding from nose (16.2%), cuts and abrasions (13.7%)
and twisting of ligaments (3.5%). There were 796 (89.3%) minor
injuries, 70 (7.9%) moderate and 25 (2.8%) severe injuries. Severe
cases of injuries resulted in concussion, internal organs damages,
third-degree sprains, eye injuries and various types of fractures.
Most injuries were related to the face (72.5%), head (11.6%) and
lower limb (6.4%). In our study in groups of karate kyokushin
athletes strongly dominated minor injuries as contusions and joint
injuries within hands and feet. The overall proportion of severe
injuries was lower than in Arriaza and Leyers study.
These differences may be since athletes analyzed by the
Arriaza and Leyers took part in the World Karate Championships
(high level of competitors), while our competitors were taking
part in the Polish and European Championships. Differences may
be also related to the dissimilarities occurring between each style
of karate. In the kyokushin style up to year 2017-foot protectors
were not obligatory for women and only obligatory protectors were
breasts protectors for women and suspensors for men. The authors
emphasize that competitive karate is associated with a relatively
high injury rate and note that cases of severe injuries were rare
what is compatible with our study. Destombe et al. [5] analyzed the
injuries sustained by the 186 French karate athletes for a period of
1 year. The study gropup consists of karatekas from three karate
clubs in Brest, France but the author did not mention the style of
karate. Total number of injuries was 83 (63 during trainings, 20
during competitions), average injuries stood at 44.6/100 players.
The most common injuries were hematomas (53%), twisting
(19%), muscle injuries (7%), fractures (7%), cuts and abrasions
(7%). Predominated limb injuries were the upper (28.9%) and
lower (35%), followed by head (26.5%) and trunk (9.6%) injuries.
Authors stress that injury rate increases with time spent on
trainings, rank of each competitor and years of practice what is similar
to our study. Destombe et al. also emphasize that serious
injuries in karate are rare. Minor injuries of the upper and lower
limbs are dominating, what is compatible with our findings. Zazryn
et al. [6] in turn, studied the incidence of injuries among professional
athletes training kickboxing for a period of 16 years. Total number
of injuries was 382, mean value of injuries stood at 109.7/1000
competitors. The most common injuries were superficial ones like
bruises, lacerations and abrasions (over 64%). Predominated head,
neck, face (51.6%) and lower limbs (39.8%) injuries, the lower leg
(23.3%), face (19.4%) and intracranial injuries (17.2%).
The nature of kickboxing where kicking the opponent is the
major movement and head is a prime object was associated with
the distributions of body regions mostly injured by participants.
The nature of kickboxing, whereby kicking the opponent is the
prime movement and the head a prime target, is reflected in
the distributions of body regions most commonly injured by
participants. Therefore, the results obtained by authors differed
from results received in karate kyokushin athletes (differences
between karate kyokushin and kickboxing style). Gartland et
al. [7] studied the incidence of injuries in muay thai kickboxing
athletes. The survey was conducted among 152 people. Mean
value of injuries stood at 13.5/1000 recreational competitors’
athletes (amateurs) and 2.79/1000 professional athletes. The most
suffered injuries were bruises, lacerations and abrasions. Among
the amateurs dominated injuries to the lower limbs (75%), trunk
(15.9%) and upper extremities (6.8%). Head injuries accounted for
2.3% of all injuries.
Among professional athlete’s lower limb injuries (53%) also
predominated. More often they experienced trauma to the head
and trunk. The most frequently occurring injuries were: bruises,
sprains, cuts and abrasions. Authors highlight that different
martial arts are associated with particular injury pattern which
may explain the differences in percentage distribution of injuries
between muay thai kickboxers and karate kyokushin practitioners.
However, worth noting is fact that, according to the authors, karate
is linked to the traumas within the lower extremities, as it can be
seen in our study. Kazemi et al. [8] analyzed the injuries suffered by
athletes training taekwondo for a period of 9 years. Average injuries
stood at 16.18/100 athletes. Predominated head injuries (19%),
foot injuries (16%) and thigh (9%). Minor traumas as: contusions
(36%), sprains (19%) and muscle strains (15%) were the most
common. Differences between Kazemi et al and our study occurred
in the distribution of rates and the leading locations of injuries.
Nevertheless, according to the authors, the most commonly
reported injuries were bruises, injuries of joints and muscles,
which is similar to our results. Kujala et al. [9] analyzed 54186
sports injuries sustained by judo, karate, football, ice hockey,
basketball and volleyball players in the years 1987-1991. Average
injuries stood at 142/1000 of karate athletes, 117/1000 of judo
competitors, 94/1000 of hockey players, 89/1000 among football
players, 88/1000 among basketball players and 60/1000 of the
volleyball players. In team games 46-59% of injuries happen during
competitions and tournaments, while in martial arts the figure was
70%. Injuries typical for each discipline predominated. Fractures
and teeth injuries were the most common among players of hockey
and karate, lower extremity injuries among football and volleyball
players and upper extremity injuries in judo. Sprains, muscle
injuries and contusions were the most common types of injuries.
The most predominant areas of the injury among karate athletes,
according to the authors’ injury were lower limbs (37.3%) -
especially: knee (11%) and foot (10.7%), and upper limbs (26.3%)
- fingers (9.3%). Other traumatic sites (36.3%) were head and neck
(10.9%). Mostly injuries (sprains, strains, bruises, fractures) were
related to the striking surfaces in karate-hand and feet joints, what
is compatible with our study findings.
Zetaruk et al. [10] investigated the incidence of injuries among
the 263 athletes trained martial arts. The survey was conducted
among athletes training: karate shotokan (114 individuals), aikido
(47 people), taekwon-do (49 athletes), kung fu (39 athletes) and
tai chi (14 individuals). Most injuries were related to the athletes
practicing taekwon-do (59%), aikido (51%) and kung fu (38%).
The least frequent injuries applied to karate shotokan athletes
(30%) and tai chi (14%). According to the authors karate shotokan
athletes suffered 114 injuries, among which the lower extremity
(22.8%), upper extremity (16.7%), trunk (14.9%) and head, neck
injuries (9.6%) were dominating. The areas of suffered injuries in
karate shotokan athletes are consistent with parts of the body that
have been injured in karate kyokushin individuals even despite
the differences in shotokan karate protector’s usage (obligatory to
compete are tibia and foot, hands protectors for athletes and breast
protectors for women and suspensor for men).
Also, Vitale et al. [13] investigated foot anatomy, anthropometric
measures, and other background factors and information as possible
risk factors of injury in barefoot athletes practicing judo, karate,
kung fu, Thai boxing, or aikido. The results of 130 subjects showed
that most of the athletes (53.8%) did not sustain lower lib injuries,
19.2% reported an overuse injury and 27.0% suffered an acute
injury. No significant differences were observed in the injury rates
in relation to style and kind of martial art. Interesting and worth
mentioning was the fact that in this study older and heavier martial
artist, performing more hours of barefoot training, were at higher
risk of acute and overuse injury. This aspect has not been addressed
in authors’ study and requires further research on a larger study
group divided into weight categories in the future. Other study
shows that even athletes who taking part in kata tournaments
(without fighting) are suffering form and overuse injury with the
occurrence of pain in the joints of the lower extremities and lumbar
spine from performing the basic stances [17].
Over the years a reduction in average number of injuries in
martial arts [11,12], including several acute injuries as concussions
to muscle and tendon ones, has been observed. Perhaps, it is due
to the widespread use of protectors, greater awareness in the
treatment area, prevention of damage and stricter enforcement of
the competitions. But it can also be caused by insufficient data. As
Thomas et al. [18] indicate that studies need to adopt one injury
definition, one data-collection form, and collect comprehensive
data for each study for both training and competitions. More data
are needed to measure the effect of weight, age and experience
on injuries, rates and types of injury during training, and for
competitors with high injury rates. RCTs are needed of interventions
such as training and feedback of performance data to reduce injury
rates. The reduction in average number of injuries can be also
caused by the changes to the safety regulations (i.e. foot protectors
in females) by members of the approvals board and medical ethics
[14,15]. The Council for Medical Ethics discourages doctors from
accepting to act as ringside doctor for combat sports that permit
knockouts or participating in approvals or appeals boards for such
events because these types of assignments in their opinion may
violate the general duty of doctors to protect human health [15].
Moreover, finding of this study considering other research
presented above are justifying a recommendation for coaches to
differ a training or accept a physiotherapist in order to prevent
injuries due to overload of ligaments and muscles as it is in
other professional sports. Martial arts did not emphasize use of
rejuvenation treatment for athletes as it is on other professional
sports, maybe due to insufficient founding in comparison to for
example football. Polish karate kyokushin athletes use all the
rejuvenation treatment individually on their own [16]. Karate
clubs do not provide such treatment. This study reveals some
information about competitive athletes and those statistics should
not be extrapolated toward all practitioners. As in many other
martial arts, people are more concern about their health and tend
to avoid injuries [19]. Such risk and special attention should be
given to those, who prepare for competitions only.
a. Most of athletes are willing to use protection of central
parts and striking surfaces.
b. Women athletes are slightly more prone to use protective
equipment than male athletes.
c. Injuries were more frequent among distal part of the body
(hands and feet) than the central ones.
d. Males suffers more back and foot injuries than women.
More BJSTR Articles : https://biomedres01.blogspot.com/