Auxiliary Device for Full-Arch Digital Scans in Edentulous Jaws
Introduction
Digital impression is not a procedure in itself but represents the first step in a “new” way of conceiving the prosthetic procedure: the digital work-flow. Intra-oral scanning (IOS), Computer Aided Design (CAD) and Computer Aided Milling (CAM) make it possible to avoid the conventional procedures with a significant reduction in production times. Digital technologies are radically revolutionising the prosthetic approach in both clinical and laboratory aspects [1-6]. To date, in implant-supported dental prostheses, scientific literature has validated the use of IOSs for capturing optical impressions for the design and manufacture of short-span restorations such as single crowns (SCs) [7-10] and partial prostheses (PPs) [11-13]. However, in case of long-span restorations, in particular full arches (FAs), IOSs do not yet seem to be sufficiently accurate, as reported by several studies [14,15] and reviews of the literature [16,17]. Although some studies claim that optical systems provide sufficient accuracy in complete-arch impressions, scientific evidence on the intraoral scanning of complete-arches with teeth is lacking and outdated [17]. Elastomeric impressions of complete arches are significantly more accurate than those of optical arches [18] and the precision of intraoral scanners decreases as the distance between each scan body increases [19-21]. As the free scanning area increases, the intrinsic imprecision of the procedure increases, with progressive distortion of the impression and, consequently, a reduction in accuracy.
Edentulous arches, in particular the lower arch, represents still today a challenge for the optical impression: it is confirmed by the evaluation of full arch scans obtained with different scanning systems compared to data obtained with traditional impression. Taking impressions using elastomeric materials to capture dental implants position is still the most widely used technique and remains the gold standard. However, the elastomeric method requires procedural shortcomings and, in addition, the technique is uncomfortable either for the patient or for the clinician [6-8]. Nevertheless, a consensus regarding the implementation of IOS in complete-arch edentulous patients rehabilitated with multiple dental implants has not yet, been established [15].
Obtaining reliable digital scans of arches where there are large homogeneous areas- between implants in edentulous arches- can be challenging, even impossible [20]. Difficulties are due to the absence of anatomic irregularities in the scanned area. In addition, Scan Bodies’ geometry can drive IOS to “interpretation errors”: scanners can recognize different Scan Bodies interpreting them as the same one [21]. Andriessen et al [21] reported that most digital scans of edentulous arches were unusable. The distance between implants also influences the accuracy of the digital scan so that longer the distance with a uniform surface is, more challenging the scanning process become [20,22]. These problems reflect IOS difficulties in matching multiple images captured during the scanning process [23]. Intraoral scanner’ software builds 3D images ‘by best-fit alignment’ of photographic frames collected by camera. The acquisition of larger areas is more challenging and software algorithm processes become more complex [23]. However, despite area’s extention, in edentulous patient, lack of differences in curvature radius leads additional difficulties. Geometric and colour differences (according to the technology used) detected by the scanner will simplify the matching process. The lack of these features in edentulous oral cavity means that digital scanning of edentulous arches is a very difficult tasks in these patients (Table 1).

Table 1: Medium distances group A and B.
To solve the problem related to intraoral scan of edentulous arches, several authors suggest several methods with the aim of create artificial anatomical references to compensate the distance between Scan Abutments; in this way, the intraoral acquisition is easier and more accurate. Some authors used auxiliary removable devices interconnecting the scanbodies (with guides, polymer bases obtained through the use of a 3D printer) [24-26]. Methods proposed in literature partially solved the problem but usually require very sophisticated procedures that often are not recommended to the traditional physical impression. To date, therefore, despite advanced technologies, in critical clinical conditions intraoral scanning can lead to non-faithful and inaccurate models.
The aim of the study is to show a new concept to improve accuracy of intraoral acquisition in all those critical cases in which the distance between consecutive Scan Abutments affects the trueness of intraoral scans. The procedure outlined in the study has the peculiar property of not requiring complex and laborious steps. The auxiliary device is made of technopolymer material (Polyether ether ketone-PEEK) and it consists in an hexagonal body connected to a settable screw. (Figure 1) The device is designed to be screwed onto a previously drilled Scan Abutment and it does not rest directly on soft tissue so oral mucosa is not covered during the intraoral scan. The chance to successfully acquire oral mucosa with devices assembled on scan bodies avoids the need to acquire two separate impressions, with and without the auxiliary deviceresulting in discomfort for the patient and in extended clinical time.
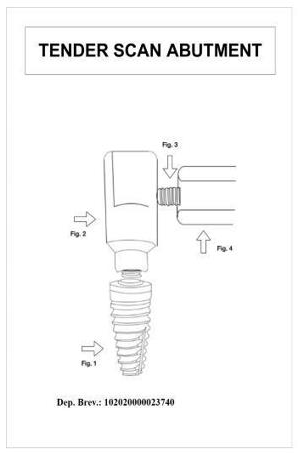
Figure 1: Design of the device.
Materials and Methods
Stereophotogrammetry technology (PIC Camera; PIC DENTAL), thanks to extraoral scanner, allows to gauge the inaccuracy associated with intraoral scanning of an edentulous arches. Gold standard STL file is acquired by indirect method by taking a physical impression, developing the cast, placing PIC Abutments on the laboratory analogues and scanning it with an extraoral scanner. Then, the gold standard is compared to STL file obtained by the direct intraoral scanning of the same arch. The ethics committee examined the research project and gave its approval to the study (ethics committee “Università Federico II” protocol no. 128/21). Patients provided written informed consent to the treatments and to the publication of the study. Written informed consent was obtained from patients for the publication of any potentially identifiable images or data included in this article.
For each of the 11 subject involved in the study three different impressions were carried out. The physical impression was performed according to “open tray splinted” impression technique using polyether material (3M Impregum Penta Soft) mixed thanks to dedicated equipment (Pentamix type). Analog transfers were pooled with self-curing resin and interdental floss. Each impression thus obtained was made into plaster cast using class 4 gypsum mixed by a vacuum- pressure casting machine. Specific targets (PIC Abutments) were placed on each transfert; then, the model was scanned using an extraoral scanner (X5 Dentsply Sirona). EOS provides an STL file where abutments are truthfully setted and we can use it as control (gold standard). Intraoral scanner (Omnicam Dentsply Sirona) is used to record two different digital impressions: the first impression is normally acquired with the only scan abutments seated (Group A) while the second impression involves the experimental device assembled as part of the “scan structure” (Group B). All digital impressions were performed by the same practitioner and all of them have been obtained according to manufacturer’s scanning protocol, starting from the distal area on one side reaching the opposite side through the occlusal area. Using a specific software (Geomagic Control X 2020) we proceed to the alignment and subsequent one-to- one comparison of the STL files obtained from IOS with the STL file obtained from EOS (Gold standard). (Figures 2 & 3) The primary measurement refers to the mean distance (average of the points dismatching between the two STL files) obtained through Geomagic 3D software. P values under 0.05 are expected to be statistically significant. Data provided by the software, expressing mean and standard deviation values either the lowest or highest distances, were summarized using standard descriptive statistic.
The null hypothesis imposes no statistically significant difference between the mean distances Group B- Gold standard and Group A-Gold standard. The comparison between the two different approaches (IOS with and without auxiliary device) is carried out by Student’s t-tests for paired samples. In the current study, the alternative hypothesis does not state direction of deviation therefore “two-tailed” test is adopted. The two-tailed test is a nondirectional hypothesis test, described as a test in which the critical region falls on both sides of the normal distribution. Thus, an alternative hypothesis is accepted in place of the null hypothesis if the calculated value falls in one of the two tails of the probability distribution (Figure 4).

Figure 2: Scan Abutment plus device in peek on the model.

Figure 3: Device in peek in the oral cavity.
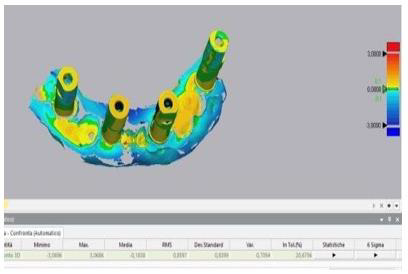
Figure 4: Comparison between stl control and stl with Commercial Scan Abutment.
Results
The two-tailed t-test for paired samples is used to test the null hypothesis that the average distances of the points made using the Scan Abutments according to the standard protocol (group A) are not significantly higher than those obtained using Scan Abutments with the experimental device (Group B). Assuming a difference of 0.1 mm between the two approaches (Group A and Group B) as clinically relevant and a standard deviation of the differences equal to 0.09 (value obtained through the evaluation of preliminary data), a sample size of 11 scans for each protocol will be enough to highlight any difference with a power of 0.9 and a two-tailed significance level of 0.05. Statistical analysis performed by using Spss software showed statistically significant differences (P <.05). Based on the results, the null hypothesis was rejected: group B values, significantly closer to zero, reflect a higher degree in their overlap with the control file. The “color maps” are used to qualitatively compare and evaluate the results: closer is the number to zero, smaller the difference between the two files is. The colors from blue to red indicate in a qualitative way the dimension of the mismatching between the file (A or B) and the gold standard control (Figures 5 & 6).
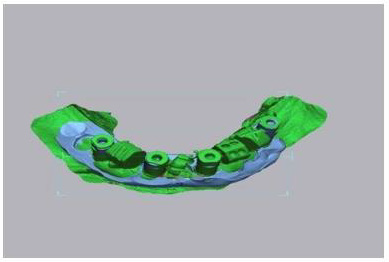
Figure 5: Alignment between stl control and stl with Commercial Scan Abutment plus device.
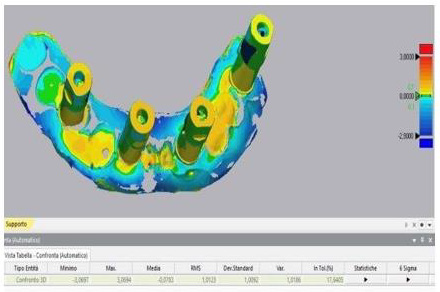
Figure 6: Comparison between stl control and stl commercial Scan Abutment plus device.
Discussion
Evidence suggests that intraoral scanning accuracy varies greatly with interimplant distance, intraoral scanner type, scan body type and operator experience. Several clinical factors can contribute to the global deviations in complete-arch intraoral scanning: the present study shows how the absence of anatomical references in edentulous arches has a negative influence on the accuracy of digital dental scans and how artifical anatomical references can be used to obtain easier and more accurate digital impressions. Limitations of the present study include the small sample size and the use of a single type of intraoral scanner. Comparison of the scans obtained with other intraoral scanners available on the market, still with the help of the device, will be reason for further research.
Conclusion
Based on the results, the null hypothesis was rejected. Full-arch digital implant impression, taken using intraoral scanners, was found to be less accurate than the same impressions recorded by the support of the experimental removable device. The present study shows how the absence of anatomical references in edentulous arches has a negative influence on the accuracy of digital dental scans and how artifical anatomical references intraoral make the acquisition in critical cases easier and more accurate.