Garlic Polyphenols: A Diet Based Therapy
Introduction
Garlic (Allium sativum L.) belongs to the family Alliaceae and has been derived from the Celtic word ‘all’ meaning pungent and nature’s boon to mankind. More than 5000 years, garlic has been used as curative and food based bioactive agent for physiological disorders. Garlic plant is mentioned in the Ancient Israel (The Talmud), Egypt (Codex Ebers), Bible and India (Vedas and Purans, Charak Sanghita). Chinese people believe that consumption of garlic as diet based therapy is most effective against human metabolic syndromes such as aging, oxidative stress, cancer, wound healing, diabetes, heart diseases and obesity [1]. Hippocrates observed that garlic was inhibited the cancer cells lines and also prevented from the intestinal and extra-intestinal diseases. Prophet Hazrat Mohammad (PBUH) recommended it for treating scorpion stings and cured health’s related disorders. In Historia Naturalis by Pliny, it was more effective against dog & snake bites as well as gastro-intestinal disorders. Allicin is sulfur containing compound formed through the action of alliinase enzyme on alliin and show the anti-platelet and hypolipidemic activity on human health. There are multiple evidences which confirm the uses of garlic as nature tonic to cure diarrhea in ancient times. In Nigeria, it is used to treat diarrhea, abdominal discomfort, respiratory tract, and otitis media infections.
In Europe, India and Pakistan, consumption of garlic was found to cure asthma, hay fever, and common colds, respectively [2,3]. Garlic is a promising source of bioactive compounds such as allicin, disulfides, alliin, allyl sulfides, cycloalliin, ajoene, allyl disulfides, methionine, cysteine, cystine, diallyl sulfides, glutathione, pseudoscordinine, dimethyl sulfides, sulfones, allyl trisulfides, thiosulfates, scordinine, methyl sulfides, tetra thiol, trisulfides cysteine, and sulfoxides [4]. It is prominent source of calcium, phosphorous, iron, nicotinic acid, thiamine, riboflavin, and vitamin C, respectively. Garlic comprises of citral, linalool, geraniol, α-phellandrene, valeraldehyde, and propionic aldehyde components [5]. They play a significant role against cancer, cataract, cardiovascular disease (CVD), hypercholesterolemia, obesity and hypertension. Maceration of garlic produces oil that good source of 3-vinyl-[4H]-1,2-dithiin, 2-vinyl-[4H]-1,3-dithiin, ajoene and allyl sulfides, whilst steam distillation of garlic oil (SDGO) gives diallyltrisulfide and diallyl disulfide [6] (Tables 1 & 2).
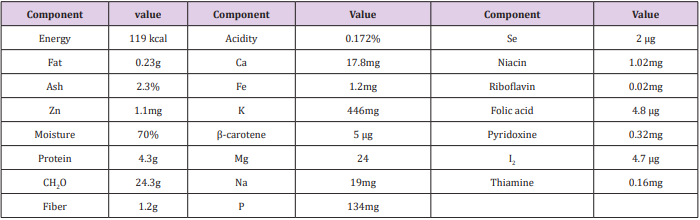
Table 1: Nutritional profile of raw garlic/100g.
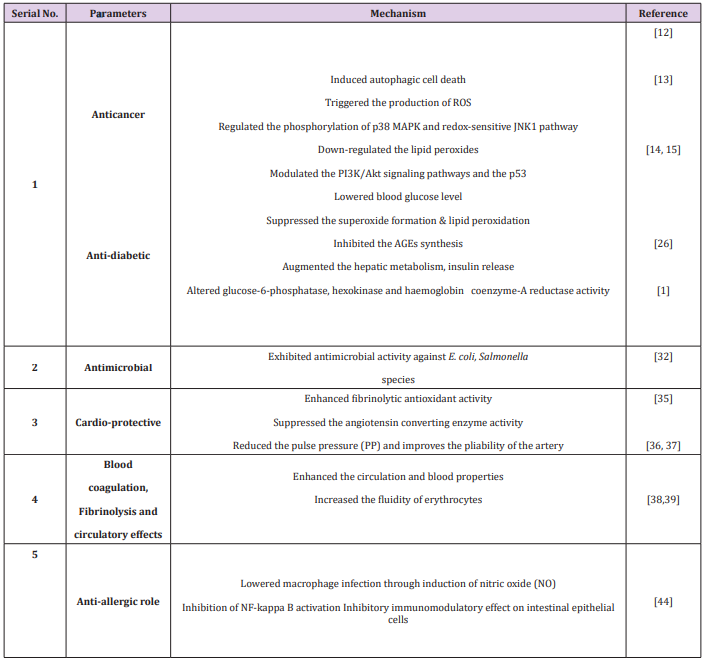
Table 2: Health perspectives of garlic.
Antioxidant Potential of Garlic
Nencini et al. [7] determined the antioxidant potential of 15% hydroethanolic extracts of aged diverse parts (bulblets, bulbs, flowers, leaves, and flower bulblets) of Allium subhirsutum L, Allium roseum L. Allium neapolitanum for 20 months. The aged garlic leaves extracts show the higher antioxidant potential followed by flowers and bulbs, whilst bulblets and flower bulblets exhibit no antioxidant potential. Nencini et al. [8] also determined the effect of garlic (bulbs or leaves, 250mg/kg) daily for 5 days in liver of ethanol induced male albino rats. They determined that garlic enhances the GSH and lowers the MDA levels, GR, CAT and SOD activities in liver injury through ethanol. Park et al. [9] evaluated the antioxidant potential garlic extracts through providing different diverse processing conditions. Aged-garlic extract (AGE) yields total phenolic contents (562.6 ± 1.92 mg/100 g GAE) as compared to heated garlic extract (HGE) or raw garlic extract (RGE). In H2O2 induced DNA damage of rats, the ED50 (19.3μg/mL) and inhibition activity (70.8%) of aged garlic extract were reported, whereas ED50 value (38.6μg/mL) of raw garlic extract for 4-hydroxynonenal induced DNA damage followed by aged garlic extract>heated garlic extract was observed. Raw and aged garlic comprises of high quantity of phenolic contents and exhibit high anti-genotoxic activity. They showed chemopreventive role against deleterious effects of H2O2 against DNA and 4-hydroxy-2,3-trans-nonenal (HNE) [9].
Health Perspectives
Anticancer Role: Garlic and garlic oil have been found to provide significant protection against N-nitrosodiethylamine-induced hepatocarcinogenesis. Garlic contains fat and water soluble sulfur compounds that exhibits the anti-cancer mechanisms through the ameliorating oxidative stress, improving immune function, and inhibiting metabolic carcinogenic activation [10]. A group of peers, Choi and Park [11] determined that garlic oil has anticancer role by inducing apoptosis, inhibiting differentiation & tumor angiogenesis and reversing multidrug resistance. Garlic is a potential phytochemical candidate against colon cancer cells, glioblastoma cells and hepato carcinoma cells. It induces apoptosis mechanism in different cancer cells. Allicin, which is the most abundant component in garlic, could induce autophagic cell death in Hep G2 cells [12]. Garlic consists of diallyl disulfide (DADS), diallyl sulfide (DAS), and diallyltrisulfide (DATS) which protect from the carcinogenesis. The supplementation of garlic triggers the production of ROS in glioblastoma cells and induces apoptosis through regulating phosphorylation of p38 MAPK and redox-sensitive JNK1 pathway.
JNK (c-Jun N-terminal kinases) is a potent inhibitor and dominantly lower the cell death by enhancing intracellular free [Ca (2+)], activating caspase-4, calreticulin, calpain, caspase-3 and caspase-9, mitochondrial release of cytochrome c and Smac into the cytosol, down-regulating Bcl-2, and overexpression of Bax [13]. Garlic dietary phytochemicals inhibit, delay or reverse skin carcinogenesis due to presence of organosulfur compounds i.e. ajoene, allicin, S-llyl cysteine (SAC) and allyl sulfides. The oral administration of garlic prevents the mice from chemical carcinogen induced skin papillomagenesis [14]. It up-regulates the carcinogenesis progression and down-regulates the lipid peroxides, as well as also modulates PI3K/Akt signaling pathways and the p53 in the skin papilloma cells [15]. Similarly, in another study conducted by Cherng et al. [16], they investigated that supplementation of DAS significantly decreased the expression of apoptotic sunburn cells, proliferative cell nuclear antigen (PCNA), UVB-induced thymine dimer-positive cells, and terminal deoxynucleotidyl transferasemediated dUTP nick end labeling whilst enhanced the p21/Cip1- positive cell population and p53 in the epidermis. Moreover, suppression of COX-2, prostaglandin E2 (PGE2), NF-κB, and NO level were reported after DAS administration, respectively [16].
There are different methods like digital rectal examination (DRE) and prostate specific antigen (PSA) use in blood sera and enhance the prostate cancer diagnosis among male population at early stages [17]. The use of androgen drugs suppresses the hormone stimulation of the prostate; on the other side, show deleterious effects on body [18]. Garlic bioactive components inhibit the proliferation of various cancer cells through the histone deacetylase (HDAC) inhibitory activity, down-regulation of the Akt and up-regulation of apoptosis of prostate cancer cells [19,20]. The earlier findings of Kim et al. [10] reported that administration of garlic compounds prevented the in vitro and in vivo rats from the prostate cancer. These compounds induced repression of the androgen receptor (AR), apoptosis, and cell cycle arrest in prostate cancer cells. Besides this, they also enhanced the histone acetylation and apoptosis in prostate cancer cells of mice [21, 22]. The administration of S-allylcysteine at the rate of 1-100 mmol/L in A2780 cells in concentration- and time-dependent fashions momentously suppressed the proliferation of cells. It also induced apoptosis, accompanying by lowering the expression of pro-caspase-3, Parp-1, and Bcl-2, and enhancing active caspase-3 and Bax. Similarly, it also reduces the migration of A2780 cells, and significantly decreases the protein expression of Wnt5a, p-AKT and c-Jun [23].
Antidiabetic Role: Diabetes is a metabolic disorder and produces the abnormal levels of glucose in the bloodstream. It is growing emerging public health problem and estimated to be 333 million people by 2025. Herbal plants are being consumed as food by the patient as well as healthy person. Synthetic oral antihypoglycemic agents are more effective to lower the hyperglycaemia level but on other side, they produce the side effects [24]. Allicin is a bioactive component and prevent from the diabetes through lowering the blood glucose level. The oral administration of allicin enhances the free amino acid content and hepatic glycogen, lowers the triglyceride and glucose in serum sucrose-fed rabbits. Similarly, the administration of garlic extracts to streptozotocin-diabetic rats reduced the sugar level, inhibited superoxide formation and lipid per-oxidation. S-allyl cysteine inhibits the AGEs synthesis [25]. DATS, AM, and DAS show the hypoglycemic action that augmented the hepatic metabolism, and insulin release [26]. Allicin controls the blood glucose level in serum and alters the activities of liver hexokinase glucose-6-phosphatase and haemoglobin coenzyme-A reductase in rabbits. It significantly increases the free amino acids and liver glycogen that lower the liver serum proteins, triglycerides level (aorta and liver) and fasting blood sugar (FBS) as compared to high sucrose-fed diet rabbits [1].
The supplementation of diallylthiosulfinate and S-methyl cysteine sulfoxide (SMCS) to alloxan diabetic rats that activates 3-hydroxy- 3-methyl-glutaryl (HMG) Co-A reductase, hexokinase, glucose-6-phosphatase, and lecithin- cholesterol acyltransferase (LCAT) enzymes [27]. Padiya et al. [28] also determined the hypoglycaemic effect of garlic that enhanced the insulin sensitivity and lowered the body weight gain in fructose fed rats. The previous findings of Osman et al. [29], they reported that daily intraperitoneal administration of allicin at the rate of 8 mg/kg diabetic experimental volunteers for 30 days. It effectively reduced the antiislet cell antibodies ICA level through following mechanism (1) the lowered pan B cell marker (CD19), lowered pan T cell marker (CD90), decreased pan innate cells marker (CD11b), prevented from the damage of langerghans islet cell.The hypoglycaemic action of garlic polyphenols could possibly due to release of bound insulin and high pancreatic secretion of insulin from β-cells. These polyphenols lower the blood glucose level, TG, LDL, VLDL and enhance the HDL level in streptozotocin and alloxan-induced diabetes mellitus rats. S- allyl cysteine restores its function in streptozotocin-diabetic rats by preventing free radicals production through modulating the NADPH oxidase. DAT lowered the fasting blood glucose (FBG), LDL and increased the HDL level in diabetic patients for 12 weeks [30].
Antimicrobial Activity: Antimicrobial drugs have failed to provide response to micro-organisms due to their expensive prices, side effects and greater risk of death [31]. The garlic containing extracts show antimicrobial activity against different types of bacteria such as gram positive (A streptococcus, s. pneumonia group, s. aureus and bacillus anthrax) and gram negative (salmonella species, citrobacter enterobacter, kilabsella and E. coli) [32]. Hindi [33] reported that thiosulfinates in garlic are responsible for the antimicrobial activity in rats. Allicin also exhibits the antibacterial action against some fish pathogenic bacteria. The 10% v/v solution of allicin in dimethyl sulfoxide (DMSO) was also showed anti-bacterial activity against aeromonas veronii, aeromonassobria, aeromonascaviae, aeromonashydrophila and streptococcus iniae. The allicin (MICs; 125 µg/ ml) concentration for aeromonashydrophila and 250-500µg/ml for aeromonas veronii, aeromonas caviae and aeromonas sobria in dimethyl sulfoxide was found to be effective [34].
Cardiovascular Role: Allicin, DATS, DADS and AM polyphenols perform their antioxidant mechanism and prevent from cardiovascular disease by enhancing fibrinolytic antioxidant activity, inhibiting platelet aggregation, reducting serum lipids and blood pressure levels [35]. The previous findings of Thomson et al. [36] reported that single intravenous dose of garlic extract (10- 100mg/kg) dose-dependently suppressed the blood thromboxane B2 concentration in rats. Garlic also up-regulates the cellular glutathione levels in vascular endothelial cells and prevents endothelial dysfunction. The prophylactic supplementation of aged garlic extract prior to ischemia reperfusion suppresses the production of free radicals and prevent from the depletion of glutathione antioxidant enzyme. Similarly, they also suppress the fibrosis development in kidney and liver organs by inhibiting the neutrophil migration. Allicin and DATS suppress the angiotensin converting enzyme activity that lowered the blood pressure and cardio-protective effect in kidney and liver. The aged garlic extract (AGE) reduces the pulse pressure (PP) and improves the pliability of the artery. Additionally, they lower the deleterious effects that produce the papilloma in the forestomach, lower erythrocytes and enhance reticulocytes [37].
Blood Coagulation, Fibrinolysis and Circulatory Effects: In oxidized erythrocytes of rats, the supplementation of aged garlic extract has been found to enhance the blood circulation via preventing hemolysis and lipid peroxidation. Allicin, AM improve the erythrocytes fluidity, whereas unable to protect the erythrocytes from t-butyl hydroperoxide-induced hemolysis [38]. They also modulate the production and function of both constricting factors (endothelin-1) and endothelium-derived relaxing factor (NO) in pulmonary arteries of mice [39]. Garlic juice and g-glutamylcysteines have been proved to show the beneficial effects on heart rate and may lower the blood pressure through inhibiting angiotensin-converting enzyme in vitro [40].
Immunomodulatory Activity: Aged garlic extract, and their bioactive components exhibit the immunomodulatory properties due to presence of organosulfur compounds. The concentration of garlic extract is dominantly effective on IL-2 and INF-γ gene expression of stimulated lymphocytes. These compounds also reduce the macrophage infection through the induction of NO production in vitro [41]. Allicin prevents from the immunemediated liver damage of T cells of mice and as well as also inhibit the NF-kappa B activation. A group of researchers [42], they investigated that allicin supplementation prevented from the intestinal inflammation though inhibitory effect on peripheral blood, and intestinal epithelial cells [42].
Antiallergic Role: Allergic responses are the activation of FceRI receptor on the plasma membrane of mast and basophilic cells is known to liberate the b-hexosaminidase, histamine, cytokines, prostaglandins and leukotrienes allergic mediators. Likewise, arachidonic acid metabolites such as prostaglandins and leukotrienes cause acute and chronic allergic inflammatory reactions [43]. Supplementation of allicin and AM can inhibit the passive cutaneous anaphylaxis (PCA) and immunoglobulin E-mediated allergic response in RBL-2H3 cells. Similarly, ethyl acetate extract of garlic polyphenols inhibits the release of TNF-a and b-hexosaminidase. They suppress the cPLA2, Syk, COX- 2 and 5-LO factors in rats [44].
Conclusion
Garlic is mainly used as commodity worldwide for its health promoting perspectives in human such as prevention from cancer insurgence and diabetes, lowering the cardiovascular complications, allergy responses, and aging. Bioactive compounds from garlic exert anti-carcinogenic potential target multiple pathways, inclusive of the cell cycle, apoptotic cell death and angiogenic pathway. The active form of alliinase enzyme can be stabilized into biocompatible materials such as alginate beads and layered double hydroxides. This review encompasses the multiple health effects of garlic and its bio-active constituents with references to health perspectives.
More BJSTR Articles : https://biomedres01.blogspot.com/