Ameliorative Role of Composite Flour Against Human Maladies
Introduction
Cereals as crops are grown throughout the temperate and tropical regions of the world and full fil the approximately fifty percent food energy requirements of population. Cereals in form of wheat, rice, maize, barley are significant source of minerals and bioactive compounds to dire human requirements. Cereals are mostly used as staple food in different regions of the world. Their grains mainly consist of three cereal grain consists of three main parts such as the endosperm (germinating seed), the germ (production of new plants), and the bran (provide protection to the grain). While, their concentrations are varied in different cereals grains with same general pattern. Wheat is the major crops after barley and oat among the cereals cultivated in the European countries and mostly consumed as staple foods [1]. Among cereals, wheat (Triticum aestivum) belongs to family gramineae and is considered second only to rice as the main human food crop. Commercially, Triticum aestivum ulgarev and Triticum turgidum durum are of most importance. It is one of substantial crop and cultivated approximately on 17% of the total land worldwide. Likewise, wheat grain is comprised of different types of tissues such as embryo portion (germ), endosperm which is fully covered by starch grains, aleurone layer (packed endosperm), and the pericarp [2].
Due to the presence of nutrients and phytochemicals, wheat become more important for the nutraceutical and functional properties. After milling, wheat has been used to prepare diverse food products such as bread for the supply of nutrients to human after milling. Wheat straw is also used as animal feed. Functional characteristics of wheat are influenced by composition, grain hardness and protein contents. Additionally, wheat also exhibits some anti-nutrional effects owing to the existence of antinutrients i.e. lectin and gluten that decrease the dysfunction and diseases in humans [3,4]. Environmental and climatic factors including temperature, humidity, topography, soil etc. affect the quality and yield of wheat productions. In industrial milling, bran is the by-product of wheat and significant nutritional profiling, health endorsing perspectives and further is also used to prepare multifarious food items [5]. Wheat is also prominent source of carbohydrates, protein, and fibers. The pericarp contains protein content (10%) whereas germ and aleurone layer comprises of 30% of the total protein. Likewise, endosperm contributes approximately 74% protein contents. In conclusion, aleurone and germ layers, endosperm relatively high protein contents [6].
Barley (Hordeum vulgare L.) is one of the most ancient cereal crops grown in the world today ranking fourth among cereal grains after wheat, rice, and maize. Barley is used as animal feed (65%), malting (33%), and human consumption (2%). It also prevents from cardiovascular disorder via decreasing the cholesterol concentrations and improving the glucose tolerance [7,8]. Mechanistically, barley flour markedly lowers the bile acids absorption, eliminates steroids, increases catabolism of cholesterol, reduces lipoprotein cholesterol secretion, enhances secretion of bile acids, and reduces the total body pool of cholesterol [9].
Chemical Composition
Considering wheat composition, wheat caryopsis is consisted of (14-16%) outer branny husk of the grain, (starch: 81-84%) central endosperm, and embryo portion (2-3%), respectively. Separation of endosperm from the embryo and bran layers are mainly done by conventional milling of wheat grains [2]. Barley flour contains higher amount of soluble dietary fibers especially ß-glucans, arabinoxylans and pectin. Barley grains is composed of higher quantity of ß-glucans as compared to other cereals. The ß-glucan contents vary from 10.89-19.7 g/100g on dry wt basis whereas this increased level is significantly used in food, feed and industrial applications [10].
The chickpea (Cicer arietinum L.) is cultivated in different regions of the world as important grain legume crop. It is also promising source of starch as major carbohydrates which is approximately 83.9% of the total carbohydrate. Chickpea seeds also consist of (21.70-23.40%) protein, and (41.10-47.42 %) carbohydrates. It also has high protein digestibility, consists of complex carbohydrates (low glycaemic index), enriches with minerals and vitamins. Chickpea flour is also free from anti-nutritional factors [11,12]. Additionally, it is also promising source of carbohydrates, minerals, proteins and vitamins and has significant role in daily nutrients intake of human. The carbohydrates and protein approximately constitute the 80% of the total dry seed mass. Moreover, dietary fiber in chickpea significantly lower the cholesterol level and also contain a variety of Anti-Nutritional Factors (ANF) including amylase and protease inhibitors [13].
Maize also known as Zea mays L. is an important Pakistani crop and it is the 3rd most cultivated crop pf Pakistan after wheat and rice. It is cultivated over a huge area in Pakistan. Mostly, maize is cultivated and produced in Punjab and Khaiber Pakhtunkhwa. Maize is consumed in different forms like in food grain form and used in different food products. It is also significantly use to form forage for utilization in livestock and poultry. It is very important as a commercial crop and contribute raw material to various industries in order to produce maize starch, maize syrup, maize oil, dextrose and maize flakes. The grain of maize constitute starch in the amount of 72%, protein in the amount of 10%, oil in the amount of 4.8%, fibre in the amount of 5.8 %, sugar in the amount of 3.0% and ash in the amount of 1.7%. In Pakistan, its area under cultivation is 992 thousand hectares and annual production of grain is grain 751 thousand tons [14].
Oat (Avena sativa) has multifunctional features and nutritional profile due to presence of components. It is a rich source of dietary fiber particularly minerals, b-glucan, and nutrients. Oats are very beneficial in the cure of diabetes mellitus and various cardiovascular diseases. The bran of oat is a rich source of vitamin B family, fat, minerals and protein, except b-glucan which is supposed to be beneficial fiber for the health of heart. This b-glucan has exceptional therapeutic properties and it is significantly important nutrient in human diet and nutrition. Diverse effects of b-glucan in terms of physiology are connected to viscosity, insulin responses, lowering the plasma glucose and enabling high movement of bile acids to lower intestine and cause high excretion of bile acid thus lowering the cholesterol level. Furthermore, it is beneficial in the treatment of celiac disease. The consumption of oat grains and oat brans in daily diet beneficial both as nutritionally and also used as therapy against many diseases [15].
Nutritional Aspects
Cereals belong to the family Gramineae and grown for their highly nutritious edible part or grain and frequently referred as grains [16]. Cereals have been consumed directly as staple foods and indirectly as feed for livestock long ago. Cereals are considered as important food sources, and foods made of cereals are supposed to be a primary energy source, vitamin B and protein, minerals for the population globally. In general, cereals are basically economical to harvest, can store and transport easily, if preserved dry it does not deteriorate readily. Cereals are used by humans since long from prehistoric times. Cereals are rich sources of macro and micronutrients and consuming high amount of cereals has significant impact by decreasing the risk of many diseases [17].
Cereals are rich source of carbohydrates and often known with the same name, because cereals consist of almost 75% carbohydrates. Starches being the chief part of cereals present in endosperm in starch granules. Starch granules contain different ratio of amylose to amylopectin which depends on the type of cereal and its variety. In general cereal varieties, amylose starch is present in the range of 25-27% although in many varieties of waxy (corn and rice) amylopectin is the chief starch present. Cereals composed of proteins in the range of 6-15% [18]. Wheat contain main storage proteins in the form of glutenins gliadins whereas rice contain glutelin (oryzenin) and maize contain prolamin (zein) while barley contain glutelins and hordeins while oats contain albumin and globulins [19]. Cereals also contribute significant quantity of good quality amino acids that are building blocks of proteins, while some amino acids are limited. Diet must provide essential amino acids and from these amino acids human body can make other nonessential amino acids. Limiting amino acids are those amino acids that are present in amount less than that is required. In case of cereals, lysine is the limiting amino acid while in rye the first limiting amino acid is the tryptophan. In rice, rye, barley and other high lysine cultivars like maize, sorghum contains favourable composition of essential amino acid. Mixture of cereals and plantbased foods like beans and rice can make up for such amino acids (limiting). Cereals contain minute quantity of lipids in the range of 1- 3% in barley, rye, wheat and rice, while oats contain 5-10% and corn contain 5-9%. This lipid is richest source of linoleic acid [20].
Cereals also contain vitamins and minerals. Cereals can also contribute to the intake of vitamin and mineral; though the content of micronutrient depends on the presence of amount of endosperm, bran and germ. Cereals do not contain vitamin B12, vitamin A & C, and no beta carotene despite of yellow corn. Though, cereals are source of significant amount of most B vitamin, particularly thiamine, niacin and riboflavin and contain appreciable amount of vitamin E. Cereals also contain minerals and are a rich source of potassium but are low in sodium like many plant foods. Whole grain cereals also comprise of iron, zinc and magnesium and minute quantity of numerous trace elements like selenium. Amongst the cereal grains, rice contributes highest level of selenium and provides about 10-13mg per 100g (Table 1) [21].
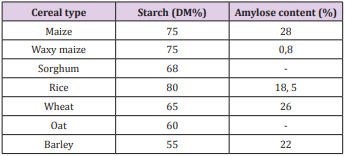
Table 1: Starch composition of cereals.
Milling of Cereals
Milling process is the process of grinding in which grind the grain into flour and significant step in post-production of grain. This technique is used to eliminate the husk, bran layers, and then produce an edible portion in form of powder with appropriate grain size. During milling, essential bioactive compounds are affected with minor alteration [22]. Categorically, there are two types of milling one is dry milling (separation of bran from the endosperm) and other is roller milling (separation of bran from wheat grain), respectively. the grains are subjected to tempering process by spraying of water to retain moisture and then shifted to tempering bin for conditioning before milling. Pericarp and germ portion of grains absorb water to soft the endosperm for extraction purposes. In addition, it also stops the breaking of bran during separation. The conditioned grains are shifted via metal rolls rotating in opposite direction during roller milling. Afterwards, the grains are transferred into three major portions such as bran, germ, and endosperm [23,24].
Regarding polyphenols, they are present approximately 20% of total phenols in bran portion of grains. The higher antioxidant activity of bran portion is due to the presence of phenolic compounds. The antioxidant compounds are significantly present in different concentrations in different parts of the wheat grains. Temperature considerably affected the rate of particle size reduction, granulometric particle distribution, and dissociation of diverse bran layers during grinding [25]. Bran layers exhibited the thermomechanical properties due to the presence of lipid compounds in the cuticles. On other side, bran was brittle, fragmented and then rapidly lowered the particle size whereas at low temperature, disruption of bran layers is low. The conversion of faster fragmentation of bran into fine particles and composite particles were done after cryogenic milling. Bran of cereals also work as an elastoplastic due to their higher high plasticity and extensibility of inner bran layers. Different bran layers also show different extensibility at ambient temperature and generated the wide range of particle sizes. The increased antioxidant potential is linked with presence of hydroxyl group of phenolic acids [26].
The replacement of wheat flour with defatted cashew kernel flour significantly enhance the fiber, fat, ash and protein contents, and energy value in the composite flour whilst lowered the carbohydrates and water contents, respectively [27]. In another study done by Igbabul et al. [28], they evaluated that product was prepared by wheat, plantain and soy in which higher protein contents significantly affect the rheological properties of bread. A peer group of researchers Méité et al. [29], they found that preparation of composite flour by mixing of wheat grains with soya bean in resulting enhanced the lipid content.
Water is an important criterion to evaluate the water quality, texture, and taste in various food products; they substituted the wheat flour with yam and vanilla flour. The low moisture contents in the flour main prevented from the growth of mico-organims and protected from the deteriorative quality of the product. In addition, low water contents enhanced the shelf life of the product [30]. Likewise, supplementation of cashed flour in wheat flour significantly increased the ash and fiber contents. The enhanced contents exert health endorsing functions such as facilitation in digestion process and prevention from the constipation. Composite flour also play role in preventing of cancer, diabetes, and cardiovascular diseases [31]. A study conducted by Brou et al. [32], they explored that substitution of cereal and legumes flours momentously enhanced the oil and water absorption potential. The enhanced water holding capacity were occurred due to higher amino acids, protein contents, conformational characteristics, and degree of interaction with water, respectively [32]. Therefore, higher water holding capacity leads to better quality of bread or chapattis by enhancing or improving the freshness of the product. In food industry, oil is absorbed in the flour through capillary process and thus acts as mouth feel and flavor enhancer [33]. Moreover, Diallo et al. [34] reported the oil absorption capacity of formulations in bread. The density of composite flour is decreased with enhanced substitution rate. Likewise, Giami [35] found that decreased density of flours linked with good formulation in infant foods. Moreover, group of researchers [36] investigated that supplementation of Treculia africana flour into wheat flour lowered the density whilst composite flours exhibited the higher mineral contents as compared to wheat flour.
Composite Flour
Composite flour is different from the ready-made mixed flour which is used in bakery products and by millers contain nonperishable constituents whereas the composite flour is the mixture of different flours of vegetables, wheat or non-wheat flour, rich in protein and starch which can be used for the production of leavened products breads, pastas, porridges, unleavened baked products, snack foods. Sometimes, only flour is used as replacement-for example, tortillas and wheat-less bread from sorghum, pastas from sorghum or maize [37]. It can be defined as combination of flours such as tubers enriched with starch (sweet potato, yam, cassava), cereals (barley, rice, buckwheat, millet and maize), protein rich flours (peanut and soy), and non-wheat flour, respectively [38]. Composite flour is promising and significant source of different acidic phenolic compounds such as ferulic acid, benzoic acid, sinapic acid, diferulic acids, and p- coumaric acid subsidiaries. Ferulic acid is the significant compound in tested grains with free, bound and dissolvable conjugated form. These compounds are present as bound phenolics and endure stomach and intestinal absorption to achieve the colon. It is also comprising of fibers, starches, proteins, B-complex nutrients, minerals i.e. Se, Zn, Mn, Fe, Mg, K, and P, respectively. Moreover, β-glucan and arabinoxylan fibers are linked with reduction in blood glucose level, coronary heart maladies, blood cholesterol, dyslipidemia, cardiovascular sicknesses, glycemic control, obstruction weight control, and ceaseless diseases [39].
Role of Composite Flours in Food Industry
Composite flour is the combination of different protein enriched foods and starches. The mostly used starches and protein to prepare the composite flour are jam, sweet potatoes as well as also peanut and soy, respectively. Different cereal and pulses are used to make composite flour including rice, millet, barley, maize, wheat, chickpea, and corn [37]. In recent years, consumers are diverted their attention towards ready-to-eat snacks due to lack of time and changes in lifestyle and eating habits. The production of composite flours to give a chance to the producers to attain and support their crops. Changes in pattern of life styles and shifting of large population to urban areas lead to enhance the consumption of flours to prepare the bread and other bakery commodities [40]. In developing economies, Oyeku et al. [41] documented that blended flours are good in nutrition and make them more economic due to presence of cheap ingredients. This phenomenon caused reduction in prices and are readily available. The supplementation of 30% legumes in composite flour significantly improve the quantity and quality of nutritious proteins that potential impact on nutritional status and economy of the country [42].
Composite flours play significant role by replacing wheat flour and are more economical by decreasing the wheat imports. This flour has role in confectionery products whereas deficient of essential amino acid in wheat and enrichment of threonine and lysine in pulse flours. Mixing of these flours make flour more nutritionally and economically. The composite foods functional characters are markedly enhanced with the increment of flours through addition of emulsion stability, swelling capacity and bulk density, accordingly. Composite flour is mainly used to enhance the nutritional values, and quality of the product in bakery products, in addition, it also prevents from the suffering from degenerative diseases associated with modern lifestyle [43]. They are also using to prepare the wheat flour by replacing the locally grown crops with higher protein contents. This substitution is also used to prepare the bread. The administration of corn (5%) in wholegrain bread to enhance the hypoglycemic role due to presence of starch, dietary fiber, and high amylase content. It also maintains the quality of bread through their organoleptic and physical properties [44].
Chickpea and wheat flour have been used to enhance the utilization of indigenous food crops whereas high protein contents with wheat flour to prepare bread. The 5% chick pea addition in whole wheat bread increases the glycemic responses owing to starch, high contents of amylase, and dietary fibers, respectively. Chickpeas bioactive compounds increase the satiation, lower the appetite and improve the glycemic index in diabetic people [45].
Health Perspectives
Hypoglycemic and Hypolipidemic
Diabetes is a chronic global disease burden affecting a large segment of population, worldwide. Various mechanisms have been involved in the progression of this human syndrome, such as pancreatic β-cell dysfunction, higher concentrations of free fatty acids, insulin resistance, leading to overproduction of reactive oxygen species, as well as pancreatic β-cell deficiency and apoptosis. The diabetes is promoted the cardiovascular disease which is linked with hyperglycemia, obesity, dyslipidemia, glucose intolerance, and hypertension [46].
In human, consumption of arabinoxylan fibers due to their soluble nature caused momentous impact on cholesterol and the glycemic index. The high viscous substances slowed down the stomach emptying and lower the motility of the small intestine that further delayed the glucose uptake. These compounds are proven effective to prevent and control the diabetes through decreasing the blood sugar level, enhancing the insulin sensitivity, decreasing the insulin resistance, and preventing from the damage of β-cells. There are linear relationships between consumption of β-glucan and reduction in blood sugar levels and glycemic index, and enhancement in insulin levels. Being potent anti- diabetic agent, arabinogalactans reduce the diabetes complications via decreasing the glucose and insulin resistance. Cereal β-glucans have physiological properties attributed to dietary fiber, such as swelling, water retention and junction, and diffusion suppression [47]. Ahmed et al. [48] recorded significant reductions in glucose levels by psyllium fibers in diabetic rats. They also found that isoflavones prevented from heart disease via maintaining physical property of arterial walls, suppressing the beta-lipoprotein -C oxidation, and proliferation of aortic smooth muscle cellular phone. Furthermore, p- coumaric acids lowered the blood lipoid levels and there was inverse relation between consumption of antioxidants and incidence of CVD [48]. The administration of wheat bran in diabetic volunteers caused momentous reduction in serum glycosylated protein levels, lipoprotein cholesterol, glycosylated albumin levels, and serum lipids levels as well as also decreased the concentrations of blood glucose. Likewise, utilization of arabinoxylan fiber markedly lowered the blood glucose level, insulin resistance, enhanced the insulin sensitivity, insulin efficiency, and provide protection from the damage of beta cells. Moreover, they also lowered the postprandial blood glucose, HbA1, low density lipoprotein and enhanced the high-density lipoprotein [49].
Composite flour has been associated with a reduction in the risk of obesity, type II diabetes, insulin resistance, hypertension, heart disease, and cancer [50]. It is enriched with higher fiber contents and recognized as to improve the glucose and insulin responses, and lower serum low density lipoprotein cholesterol through enhancing digest viscosity and embedding to bile acids in the small intestine. These bindings are linked with reduction in absorption of sugar and lipids. The insoluble fibers significantly lower the blood pressure and glucose levels in human volunteers [51]. In gastrointestinal tract, bacterial fermentation of nondigestible cereals components is directly responsible for the antiinflammatory role, anti-diabetic role and cardio-protective [52]. A study explored by [53], they investigated that whole-grain diet enhanced the diversity and number of intestinal microflora as well as also showed metabolic and immunological improvements in healthy subjects [53]. Likewise, composite flours of different cereals also have been found effective against multiple human syndromes such as obesity, diabetes, cardiovascular disease, diabetes and obesity in human [54].
Effect of Intake of Composite Flour on Renal Functions
From muscle activity, creatinine is a waste product in the blood. Creatinine level becomes higher in the blood after slowing down functions of kidney. In kidney patients, whole grains-based diet should be reconsidered. Low bioavailability of whole grain phosphate is linked with high phosphate content and phytase enzyme. This enzyme is responsible to release the phosphorus from the phytate. In kidney patients, the diet should be required to give fiber contents along with health benefits and provide sufficient protein without raising the phosphorus level. Prolamines are main wheat storage protein due to higher proline and glutamine amino acids. The prolamins categorized into three groups: (i) high molecular weight glutenins, (ii) low molecular weight glutenins, and (iii) sulfur-rich gluten subunits [55,56]. Wheat polyphenols provide protection against oxidative damage induced by carbon tetrachloride. These bioactive compounds in cereals mitigate the lipid peroxidation and the restore the healthy kidney tissue through inhibiting the free radical production and enhancing the antioxidant enzymes activities. They have potential to initiation of radical chain reaction by deactivating the reactive free radicals [57]. Cereals compounds are promising source of saturated fatty acids and unsaturated fatty acids which exhibited anti-inflammatory role by lowering free radicals’ development and Nicotinamide Adenine Dinucleotide Phosphate (NADPH) oxidase activity [58]. In addition, they also protect the body organs by reducing the pro- oxidation. In conclusion, therapeutic potential of these compounds has been found on acute renal damage [59].
Foods originating from animal sources meat, poultry, fish, eggs and dairy products are all high biological value protein foods; soya is the only high biological value food originating from a plant. Soya beans can be used as whole beans or soya sprouts, or processed as soya milk, tofu, tempeh, soya sauce or miso. The administration of wheat- soy breads (100%) and hard wheat bread (100%) have been found effectual to decrease the serum level of urea, creatinine and total bilirubin in experimental subjects after 4 weeks [60].
Oxidative Stress
Oxidative stress is imbalance between oxidative (production of free radicals in human body) and anti-oxidative systems of the cells and tissues. Thee free radicals embedded with lipids, proteins and nucleic acid which further linked with changed cell signaling, loss of energy metabolism, altered cellular transport mechanisms, cell cycle control, and genetic mutations as well as also lowered the biological activity, immune inflammation and activation [61]. Diabetic retinopathy remains the main source of visual deficiency in working-aged adults the world over. The diabetic macular edema and diabetic retinopathy are the serious vision compromising phases of the confusion. Hyperglycemia, oxidative pressure and provocative pathways are the vital segments that are ensnared in the prevalence of diabetic retinopathy [62].
Whole grain oats secure the body against age-related ailments, for example, and diabetes, cardiovascular maladies. The presence of micronutrients and fiber in different parts of wheat grain (germ and external layer) provide protection against oxidative stress. They also curtail the diabetes, obesity, and inflammations disorders. Whole grains are good and enrich source of bioactive compounds such as phenolic acids, zinc, iron, copper, selenium, manganese, phytic acid, lignins, lignans, and alkylresorcinols. All these compounds have effectual role against different types of human cancers and various syndromes. In vitro and in vivo studies, they also neutralizing or scavenging the effects of free radical production. In addition, it also enhances the cell reinforcement status due to the presence of choline, betaine, and sulfur amino acids [63-65].
Conclusion
Cereals are promising and prominent source of bioactive compounds and have been found effective to curtail various human disorders such as hyperlipidemia, obesity, diabetes complications, cancer insurgence, and cardiovascular disorder. They are good source of ferulic, p-coumaric acids polyphenols, vitamins, minerals, and arabinoxylans. The composite flour preparing by lentils, chickpea and guargum exhibited significant hypocholesterolemic effect via lowering cholesterol levels, low density lipoprotein and triglycerides concentrations, suppressing LDL-C oxidation, proliferation of aortic smooth muscle cells, and maintaining of the physical properties of arterial walls, respectively.
For more Articles on : https://biomedres01.blogspot.com/