Unplanned Pregnancies and the Consequences Among the Garment Workers Around Dhaka City
Introduction
Over the past 35 years, the growth of the garment industry has changed dramatically, and recent financial report shows that 80% as Bangladesh’s total foreign earning foundation. There are now 4,825 garment factories in Bangladesh and they are now creating job over three million people. The majority of the workers are women (85%), in which employees are able to give an amount of time and efforts to their work and also their personal life outside the work (Anna [1]). The Economist commented on this trend claiming, “Women’s empowerment in economic sector is debatably the biggest social change of times” (Anna, et al. [1]). Over the last decade, economic pressures have significantly raised the need for dual-earner families (Ford, et al. [2]). Additionally, into the paid work force, it has either directly or indirectly affected almost everyone in the society (Jenkins, et al. [3]). For every pregnant woman who dies during the childbirth, also around twenty more women suffer from injuries, infections or diseases which account to nearly 10 million morbidity in each year (WHO, 2013). Unsafe abortion is the major causes of deaths of mothers among other causes, and it accounts for nearly 13 percent of deaths (WHO, 2013). The decreased rate of Maternal Mortality Ratio (MMR) by half since 1990. The rate of MMR in developing countries is till 15 folds higher than the developed countries (UN, 2013).
Every year in the developing countries about 184 million child bearing mothers occur and among them 40% of these are unwanted (Bongaarts, et al. [4]). It is considered that about partly of the accidental pregnancies are mostly wrecked in termination, reason for maternal deaths at least one in seven globally (Singh, et al, [5]). Most of these deaths (approximately 95%) occur in developing worlds (Ciment, et al. [6,7]). It is designed to know pregnancy intention assessments of a woman’s plan before getting pregnant and also worried about the family planning issues. Accurate calculations that are valid for a diversified population is necessary (Gipson, et al. [7,8]). According to the National Survey of Family Growth (NSFG), unwanted pregnancies are whether “mistimed” or “unwanted” and it is calculated by retrospective questions which are assessed by the timing and intension for children. Diversification in pregnancy intention gauging between survey tools and continuing adjustment of assessments make contrasting results between surveys difficult if possible (Petersen and Moos, 1997, Fantahun, et al. [9,10]). Bangladesh is a developing country. It’s economy depend on the readymade garment industries. Majority of the workers in garment factories are 80-85% are women, they are not well educated and most of them are the victims of childhood marriage. So, they became pregnant at the very young age. Due to economic constrains they are forced to do jobs in garment industries. Their irregular use of contraceptives caused unplanned pregnancies in most of the time. In Bangladesh there are limited number of studies that were done on unintended pregnancy. Universally, 38 % of pregnancies are unwanted. At the international level, the rate of mortality of mothers (MMR) decreased by under 5.5 % to accomplish the aim of MDG (Siddhartha, et al. [11,12]). All the 8 goals of MDGs, nations have made the slightest improvement on the way to maternal mortality reduction (US Global Health Policy, [13- 25]).
Justification of the Study
Maternal benefits given by the Factory: The aim of this study was to determine the consequences of unplanned pregnancy among female garment workers in Dhaka city. For this study purposes, both pregnant and non-pregnant women who had history of previous abortion were included. This is the crucial factor that plays a great role in unintended pregnancy. As this benefit is maintained by the Bangladesh government so, the factory is compelled to maintain this. Therefore, this study was executed to determine the occurrence of unintended pregnancy and factors which are associated among randomly selected pregnant and non-pregnant women in readymade garment sector of Bangladesh.
Methods and Materials
Study Locale
The study was carried out in New Age Apparels Ltd. in Ashulia, Dhaka, Bangladesh. A cross-sectional descriptive research design study was conducted from September 2019 to November 2019. Basically, the study targeted all women who were having history of both intended and unintended pregnancy and also history of termination. Total 123 female garment workers were interviewed based upon a structured questionnaire. Among the study population, 100% of them were married and had the idea of family planning and methods were available for contraception. Their age average 24.3 years ranging from 18 years to 36 years. Total 123 female garment workers were interviewed based upon a structured questionnaire. Among the study population, 100% of them were married and had the idea of family planning and methods were available for contraception. Their age average 24.3 years ranging from 18 years to 36 years. Structural questionnaire was used for correlation of necessary information and medical record review were done for the assessment of the health of the female garment workers.
Ethical Considerations
It is a set of moral principles which maintain the integrity of the research and guide researchers how to deal with participants effectively (Mack, et al. [26-45]). Additionally, permission was taken from Institutional Review Board (IRB) of American International University-Bangladesh (AIUB), the committee on activities involving human subjects.
Results
Demographic Information of the Respondents
Most of the garment workers were experiencing at least 2 number of pregnancies. Minimum was 1 and maximum was 4. The female workers (52%) were on contraceptive methods and among them only 8% were regular and rest of them were irregular and thus they were witnessed unintended pregnancies, around 63% were having financial crisis and their job duration ranging from 1 year to maximum approximately 18 years (Table 1). The determination of the age at 1st birth of female workers were nearly 19 years and minimum age of 1st conception was 16 years and maximum was 27 years. Determination of intended pregnancy was around 32% and unintended pregnancy was 68% (Table 1). Among them the determination of keeping the baby was 59%. Those who were facing unintended pregnancy, the determination of termination of the pregnancy was 39% (Table 1). The total number of pregnancy was 75% among the population of the study. Rest of them were non-pregnant because they already did their abortion and came to medical room which was situated inside the factory. The determination of age of last child ranging from 0 to 15 years (Table 1).
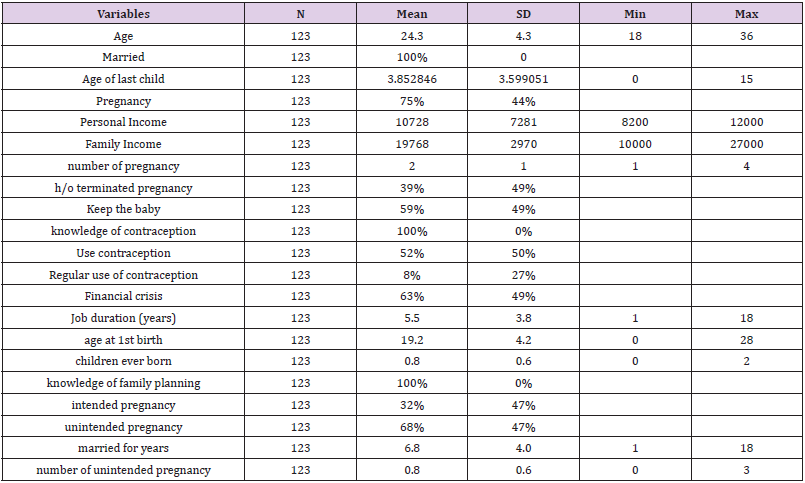
Table 1: Descriptive characteristics of the study population, (N=123).
Pregnant and Not-Pregnant Workers for Continuation of Pregnancy
Overall responsive behaviors regarding keeping the baby among female garment workers were satisfactory, 20 women who were pregnant, did not want to keep the baby and they went for abortion, not to keep the baby were 51 and 72 were interested in keeping the baby. Totally 92 female workers were pregnant. The Chi-square test value is significant at 1% level. Here the study showed that majority female workers were interested to keep the baby because they will get maternal benefit from the company as well as they will not lose the job (Table 2).

Table 2: Significant difference between who wants to continue and abort the baby.
Different Methods of Contraceptives Used by Female Garment Workers
Approximately 47% female workers were on no methods and the frequency was 58, 29% women used contraceptive pills like shukhi, famicon, minipills and so on but they were not regular on their pills. Only 16% workers used injectable contraceptives , last only for 3 months and moreover and not regular on that method too. Only 8% women’s husbands used condoms as contraceptive but mostly failed to give full contraception because the failure rate was higher and the rupture of condom was common. The Female workers (52%) were on contraceptive methods and among them only 8% were regular and rest of them were irregular and thus they were victim of unintended pregnancies, around 63% were having financial crisis and their job duration ranging from 1 year to maximum approximately 18 years (Table 3).

Table 3: Percentage and frequency of use of different types of contraceptive methods.
The Percentage of Children Ever Born
Majority (63%) of the female workers experiencing 1st pregnancy, 24% female workers reported that they had one alive child (Figure 1). Only 13% female workers had two alive children and their present pregnancy was third pregnancy.
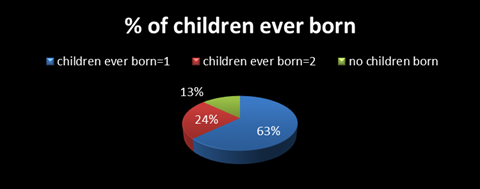
Figure 1: Percentage of children ever born.
Intention of Mother to Get Pregnant
Most of the female workers do not want to get pregnant as they think they might loose their job. So, nearly 68% of female garment workers were experiencing unintended pregnancy. On the other hand around 32% women were intentionally want baby and they continued their pregnancy.
Consequence of the Pregnancy
There were two consequences of unintended pregnancies, Either they terminate the child by using the different methods of abortions or they continued their pregnancy. This present study showed, almost 60% women continued their pregnancy and rest of the women (40%) terminated their pregnancy.
Causes of Termination of Unintended Pregnancy
About 55% female workers who wanted to keep the baby. Here both intended and unintended women were involved. Financial crisis played a major role in workers lives. Female workers who were facing economic crisis (about 26%), did not want to keep the baby. And they prefer to terminate the baby in the early stage of life. Another common issue not to keep the baby was domestic violence, like husband verbally and physically abuse the woman, to keep the wives salary. The least common cause of abortion was husband or his family members did not want the child to be born. Approximately 8% women abort their child by the pressure of her husband and in-laws. The reason behind that couples were newly married and also economic insolvency (Figure 2).
Complications and Hospital Admissions During the Termination of Pregnancies
It was observed that, approximately 60% (N= 74) female workers did not face any complications so, there was no need for hospital admission. The major reason for that was they were not terminated their baby. But nearly 38% workers who did not want to keep the baby they faced complication during the abortion. The number of women N=39 who were facing complications during abortion and majority faced bleeding problem. On the other hand, only 8% (N=10) female workers did not face any complications during that process so, they did not need any hospital admission (Table 4).
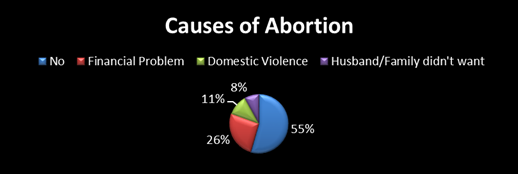
Figure 2: Of termination of unintended pregnancy.

Table 4: Complications and hospital admission ratio.
Methods of Termination of Unintended Pregnancy
Those who were used different methods for doing termination of pregnancy like menstruation regulation (MR), they were hospitalized. Also, those who were on herbal pills or took herbal method faced complications and thus admitted into the hospital. Among the study population admission during the study period. any hospital nearly 14% (N=17) female workers admitted into the hospital. Only 27% (N=33) did not require termination. Approximately 59% female workers who were not pregnant that time or primi gravida and wanted to keep the baby and also had unintended pregnancy. Another method used to abort the child was use of herbal products from some local kabiraj and from unskilled dhais. Herbal products used approximately 7% garments workers (Figure 3). This (Table 5) shows the correlation among the variables. The higher value shows that there is high correlation. The positive value shows that there is positive correlation between the variables. For example, the value -0.51 shows that there is negative relationship exist between keep the baby and number of unintended pregnancy and the correlation value is 0.51. So, it shows a good correlation. It also shows that the personal income is -0.10 and there is a negative relation with the number of unintended pregnancy and the correlation value is 0.15. So, if the personal income is high the tendency of continuation of pregnancy is lower. Again when the family income is good (correlation value 0.06) then the number of unintended pregnancy become lower (-0.13). Moreover, there is a negative relationship between financial crisis and continuation of the pregnancy. If financial crisis is present, the rate of continuation of pregnancy decreases (Table 6). Another good correlation is seen from the (Table 6) and that is the job duration and the continuation of the pregnancy. The correlation value of job duration is -0.04 and the continuation of the pregnancy is 0.07. Here shows a good correlation between them.
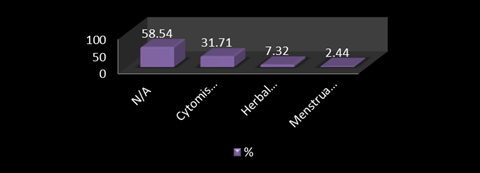
Figure 3: Methods used for termination of unwanted pregnancy.
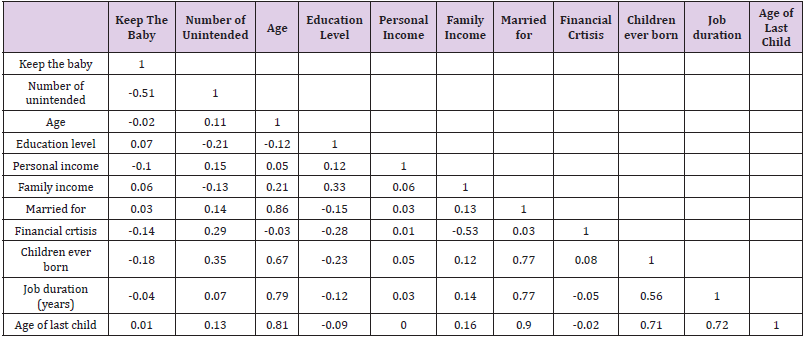
Table 5: Relationship of different financial factors, no. children, unintended pregnancy and keeping the baby.
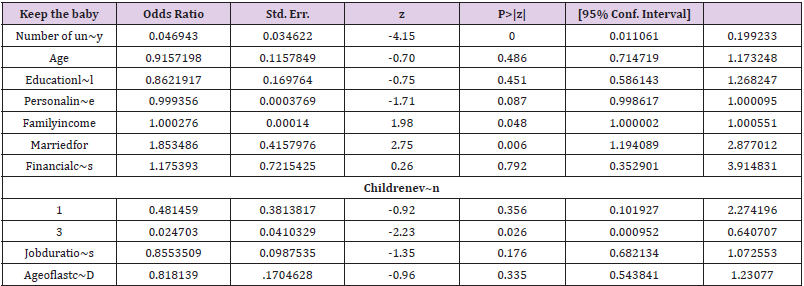
Table 6: Multivariate logistic regression model.
Note: 1 failure and 0 successes completely determined
Logistic regression
Number of obs = 123
LR chi2(11) =54.17
Prob>chi2=0.0000
pseudo R2=0.3245
Log likelihood=-56.370247
Source: All calculation based on collected data
There is no relationship between the garment worker’s age and the unintended pregnancy. Both this group has the same age irrespective of their intended or unintended pregnancy status as the P-value is not significant. The mean value of ages of female workers both who wanted pregnancy and unwanted pregnancy are almost same and that is 24 and even the 95% coefficient interval value was same as 23 (Table 7). The regression equation is specified as keep the baby as a function of the other explanatory variables such as number of unintended pregnancy, age, education level, personal income, family income, years of marriage, financial crisis, number of surviving children, job duration and the age of last child. The dependent variable is binary (keep the baby: Yes=1, No=0). As the dependent variable is binary, so, need to apply logistic regression model and get the odds ratio (OR), have run log it regression model and got the odds ratio in STATA software (Table 6).

Table 7: Relationship between age and unintended pregnancy.
Note: diff= mean(No)- mean(Yes)
Ho: diff=0; t=0.5965 degree of Freedom=121
Ha: diff<0
Pr(T < t)=0.7240;
Ha: diff !=0
Pr(|T| > t) =0.5520;
Ha: diff>0
Pr(T > t)= 0.2760
Discussion
The plan of this learning was to establish the frequency and factors linked with not deliberate pregnancy among women who are at this time working in garments factory. The cram was limited in one garment factory in Dhaka city. More than half of the respondents has their current pregnancy unintentional. Result indicates that age of women, educational status of women, economy of the household, children ever born, history of terminated pregnancy, maternal benefits given by the factory were significantly associated with unintended pregnancy.
Adult women were more to be expected to experience unintentional pregnancy and they were more wished-for continue the baby. The amount of money they got from company as maternal benefit was really high. Younger women who already had one baby, they were less interested to have second baby so early. Still financial constrain played a major role in case of keeping the baby or not, the amount of money they got from company as maternal benefit and also after returning from their maternal leave they still had their job in the same position. So, though it was an unintended pregnancy, they still wanted to keep the baby rather than terminate it. However, women who got high salary were less likely to have their second baby. Because they got high salary annually but the maternal benefit amount was really low in comparison to their salary.
Workers who were newly married, they were more prone to terminate their 1st pregnancy because their family did not want baby so early. An additional very vital issue was, every women knew about contraceptive methods and they mostly dependent on pills. Although they were not regular on their pills or other contraceptive methods like injections, implants and condoms etc. Hence consequences in unexpected pregnancies. Women who had history of termination or wanted to terminate the baby, they mostly used cytomis pills, iron pills or some other unknown pills which were taken from local pharmacy. Only a few number of women went to hospital and did menstruation regulation (MR). Some of them used herbal products for termination of pregnancy and when they faced problems , they got admitted into hospitals. They were not interested to go to hospitals for termination because of financial constrain. Wealth index was found to be significantly associated with unintended pregnancy in all models. However, there is difference in strength of association within different categories.
Conclusion
This revise is paying attention on the verdicts the prevalence of unintended pregnancy and factors associated with unintended pregnancy in garments sector in Dhaka. Results reveal that more than half of pregnancies are unintended, which is a very challenging issue. Age of women, economic condition of the family, educational status of women, numbers of previous births and history of terminated pregnancy and maternal benefits given by the factory were found to be significant associated with the pregnancy intention of women. In conclusion, from this study many factors contributed to the unintended pregnancy. It is understandable that the figure of earlier children a woman has had is a discrete determinant of whether or not the pregnancy is needed, or required at the time of conception. Further births enhance the possibility that a pregnancy will be useless and also amplify the probability that a pregnancy will be untimely. It may as a result of being effective to spotlight family setting up campaigns more intensively on those families that by now have two or more offspring. Overall, there is a substantial demand among women who are working in garments for effective contraceptive methods which are mentioned in this thesis. Women with additional children and women with abortion should be acknowledged and straightforward admittance of contraceptives information related to contraceptive use should be provided to them. In this way newborn and maternal death and morbidity as well as the need for abortion are decreased and the overall wellbeing of the family is maintained. In Bangladesh there is still carry out the early marriage whereas in some communities even child marriage is adept. Delay in age at matrimony shifts the time for sexual activities especially in the Bangladeshi context, therefore, government should address the issue of early marriage by investing in proper education and women empowerment.