The State of Central Hemodynamics in Patients with Neuroischemic Form of Diabetic Foot Syndrome is Associated with Chronic Heart Failure
Relevance
As is known, cardiovascular diseases(CVD) are the leading non-violent deaths in the world. At the same time, coronary heart disease (CHD) is leading among CVDs. So, according to the authors, in 2020 it affected 126 million people worldwide, which is 16% of all deaths [1]. men suffer from coronary artery disease more often than women[1]. According to WHO, mortality from coronary artery disease is highest in Russia, Ukraine and USA [2]. According to Rosst at, in 2018, 28.4% of all deaths in Russia were due to coronary artery disease [3]. The clinical manifestations of coronary artery disease are varied and include: asymptomatic myocardial ischemia, angina pectoris, acute coronary syndromes (unstable angina, myocardial infarction) and sudden cardiac death [4]. Definitions and classifications of types of CAD may vary between countries and guidelines, but a common criterion is the degree of narrowing (stenosis) coronary artery [5].
There are three types of coronary heart disease:
a. Obstructive: blood vessels are severely constricted (≥50%) or blocked.
b. Non-obstructive: Blood vessels constrict (<50%) because they branch into smaller vessels or due to the way the heart muscle works.
c. Spontaneous dissection of the coronary arteries i.e. rupture of blood vessels in the heart [6].
Cardiovascular disease is often associated with type 2 diabetes mellitus (T2DM) and can become life-threatening, especially coronary disease, stroke, and heart failure. Their clinical picture is sometimes atypical and asymptomatic for a long time. Type 2 diabetes should be considered as an independent cardiovascular risk factor. In this series, diabetic foot syndrome (DFS) is a severe complication secondary to microangiopathy, microangiopathy, and neuropathy. It can be considered as a super complication of several complications [7]. Elevated triglycerides have been shown to be an independent risk factor for lower limb amputation in diabetic patients [8]. Most patients with diabetic foot ulcers also have insulin resistance, central obesity, dyslipidemia, and hypertension, which characterize the metabolic syndrome, which in turn is associated with an increased risk of serious cardiovascular events. According to a German-Austrian multicentric study in 2017, new concepts are needed to prevent amputations caused by DFS and to reduce cardiovascular risk factors before the onset of DFS. Hypertension, nephropathy, peripheral vascular disease, stroke, or myocardial infarction were more common than in patients without DFS (all P<0.0001) [9]. Several studies have reported that rates of mortality and morbidity from cardiovascular disease are 2 to 4 times higher among patients with type 2 diabetes than among non-diabetics. Various studies also show that foot ulcers in diabetic patients are associated with higher mortality. In fact, diabetic foot is the main cause of morbidity in patients with type 2 diabetes, and the mortality rate is approximately twice as high as in patients without foot ulceration [10-12]. In a study [13] by Pinto et al., these authors hypothesized that type 2 diabetic patients with DFS may have a worse prognosis in terms of faster progression of cardiovascular damage and higher cardiovascular morbidity.
They showed a higher prevalence of the main cardiovascular risk factor, subclinical CVD markers, and previous and new cardiovascular and cerebrovascular events in diabetic patients with foot complications. At the same time, there are practically no works in the literature devoted to the study of issues of peripheral vascular hemodynamics in patients with DFS associated with IHD and CHF. However, we did not find in the available literature data on a comprehensive assessment of the microcirculatory bed (MCR) of the vessels of the lower extremities, which allow us to determine the nature of changes in micro vessels in patients with neuroischemic (NI) form of DFS, and coronary vessels of the heart, brain, which is of great interest. The conducted retrospective analysis reported that the diagnosed severity of primary diabetic ulcer is the main predictor of mortality, despite the risk of death from transient ischemic attacks (TIA), strokes, coronary heart disease (CHD) and peripheral arterial atherosclerosis. Despite the progress made in the treatment of ulcerative defects in DFS over the past 25 years, the survival rate in this group of patients remains low. The organization of interdisciplinary interaction is necessary for the implementation of care for patients who have undergone amputations of the lower extremities, which are carried out in the age period of 50-80 years [Gurieva I.V., 2001]. Of course, today an integrated approach to the treatment of SDS requires the provision of timely medical care in a single specialized and multidisciplinary institution, as well as improving the evidence base for evidencebased interventions [Jeffcoate WJ et al., 2018]. All of the above motivated the present study.
Purpose of the study
Study results of ultrasound dopplerography of the heart in patients with neuroischemic form of diabetic foot syndrome associated with chronic heart failure.
Material and Research Methods
During 2022, we examined 64 patients with DFS in the neuroischemic form on the basis of the Department of Surgery of the AndesMI. The patients were divided into 4 groups: 1 gr -patients with type 2 diabetes and neuroischemic form of DFS and CHF– 15 patients, group 2 - patients with type 2 diabetes and neuroischemic form of DFS without CHF - 18 patients, Group 3 - patients with type 2 diabetes and neuroischemic form of DFS, CHF and dyscirculatory encephalopathy stage 2-3 - 16 patients. group 4 - persons with CHF without type 2 diabetes - 15 patients. All patients were subjected to general clinical, biochemical (glycemia, glycated hemoglobin, PTI, ALT, AST, bilirubin, urea, blood creatinine), hormonal (IRI, C-peptide, inflammation marker-pro-inflammatory cytokine TNF-a, vascular endothelial growth factor (VEGF-A),and instrumental research methods - Doppler ultrasound of the vessels of the brain, lower extremities, ECG, Echo-ECG, bacteriological analysis of discharge from the wound, as well as statistical methods. The obtained data were processed using computer programs Microsoft Excel and STATISTICA_6. Differences between groups were considered statistically significant at P<0.05. Mean values (M), standard deviations of means (m) were calculated Significance of differences in the level between rgroups was estimated by the value of the confidence interval and Student’s test (p). Differences were considered statistically significant at p<0.05.
Results
Table 1 shows the distribution of examined patients by sex and age. As can be seen from Table 1, patients in the age group from 45 to 74 years prevailed, both among men and women - 30/17 cases, respectively. Table 2 gives initial clinical characteristics of patients of the studied cohort – patients of the studied groups. As can be seen from Table 2, there were no special clinical and anamnestic differences in the groups. Among the risk factors, hereditary burden for DM dominated - only 21 cases out of 60 (35%), smoking - only 49 cases (81.6%), alcoholism - 16 cases (26.6%). The next step in our research was to study indicators of structural and functional parameters of the heart in patients (Table 3). As can be seen from Table 3, there is a significant difference in the indicators of central hemodynamics in the studied groups compared with the norm: for example, LV EDR, ESV, EDV, LV ECR(p<0.05), mean pulmonary artery pressure, early diastolic filling blood flow deceleration time, LVTL (p<0.001), EF, ratio of peak E and A wave velocities, LV isovolumic relaxation time, LVMI, LVMI (p<0.001) 0.05). Thus, in patients of the studied groups, significant deviations of the Echo- ECG, which requires further study.

Table 1: Distribution of patients by sex and age (WHO, 2017).
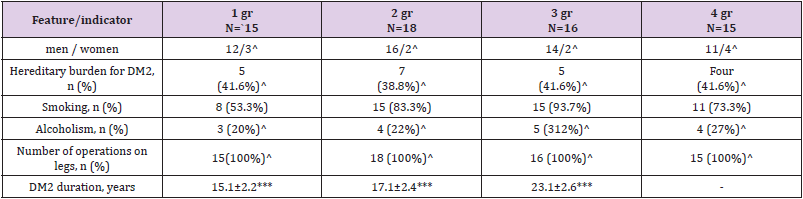
Table 2: Clinical and anamnestic characteristics of patients included in the study.
Note: *-p<0.05 with groups 1 and 2., ** – p<0.05 with groups 2 and 3, *** p<0.05 with groups 1 and 3. ..^ - p>0.05
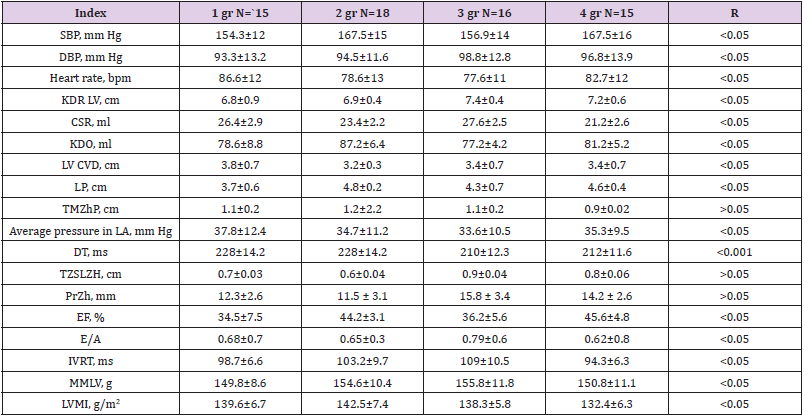
Table 3: Indicators of structural and functional parameters of the heart in patients included in the study (M ± m).
Note: *Differences are significant, p < 0.05, < 0.001 in comparison with the norm.
Conclusion
one. Among the risk factors, hereditary burden for DM dominated - only 21 cases out of 60 (35%), smoking - only 49 cases (81.6%), alcoholism - 16 cases (26.6%). 2) Significant deviations of central hemodynamic parameters were revealed in the studied groups.