Real-Time Tissue Elastography in Epidermal Cyst: along with Enhanced MRI and Elasticity Features of Peripheral Rim
Introduction
In recently years, dermatologic ultrasound imaging has been rapidly developed [1]. DERMUS (Dermatologic Ultrasound), the international working group, was formed and provided the guidelines for performing dermatologic ultrasound examinations [1] and proposed for an assessment training program [2]. Epidermal cyst are common benign subcutaneous lesions known to result from progressive cystic ectasia of the infundibular portion of hair follicles [3]. Epidermal cyst also develops in hairless skin such as planter and palmer. A different pathogenesis was suggested in the occurrence in hair follicles and in hairless skin namely palmoplantar location. It is sometimes difficult to distinguish an epidermal cyst from other benign skin tumors, such as lipoma, ganglia, pilomatricoma and dermatofibroma. Meanwhile, asymptomatic unruptured epidermal cysts need no treatment, whereas ruptured or infected cysts should be surgically removed [4].Therefore preoperative correct diagnosis is important, and different treatment options should be planned for ruptured and unruptured cysts [5].
Real-time sonoelastography is an ultrasound-based technique using the property that the tissue strain due to compression is lower in hard tissues [6]. Real-Time Tissue Elastography (RTE) is widely used for diagnosis of breast [7], thyroid [8] and testis [9] on tissue elasticity. With respect to the differentiation the ruptured from unruptured, characteristic features on gray-scale Ultrasonography (US) [10,11] and color Doppler US [11,12] have been reported. The author previously reported that the comprehensive procedure using high-resolution ultrasound is useful for the accurate diagnosis of epidermal cyst [13]. The studies have been reported on RTE of epidermal cyst, using RTE [5,9,13-15] and Shear-Wave Elastography (SWE) [16]. In this article, the current knowledge of epidermal cyst on RTE along with enhanced MRI and elasticity features on RTE of peripheral rim will be reviewed in detail. The author also will describe the differentiating ruptured from unruptured epidermal cyst with an emphasis of the peripheral rim.
Dermatologic Ultrasound
Dermatologic ultrasound imaging has been rapidly growing in recently years because of the development of high-resolution multifrequency transducers and multichannel color Doppler machines [1]. DERMUS proposed that the minimum frequency recommended for performing dermatologic examinations was 15 MHz [1]. We usually perform US tests for dermatologic diseases with a high-resolution, broad-band (5MHz-18MHz) linear transducer (Nobulus Hitachi, Ltd.Tokyo, Japan). Until now we have reported many studies in the dermatologic field [13,17-22].
Pathogenesis in Epidermal Cyst
Epidermal cyst are common benign subcutaneous lesions known to result from progressive cystic ectasia of the infundibular portion of hair follicles [3]. While in hairless skin such as planter and palmer regions, it has been proposed that palmoplantar epidermoid cyst may be related eccrine ducts and that human papillomavirus (HPV) 60 may play a role in their pathogenesis [23]. It has been also reported that palmoplantar epidermal cyst may develop when infected by HPV 57 or 60 [24]. A different pathogenesis was suggested in the occurrence in hair follicles and in hairless skin. The imaging appearance of HPV-associated plantar epidermoid cysts on MR and US has been reported [25].
Gray Scale Ultrasonographic Appearances
It has been reported that epidermal cyst on gray-scale US shows 2 types as pseudotesis and nonpseudotestis [26] and the report of the classification of 5 patterns have been described [27]. Unruptured cyst shows round-to-oval shape, posterior echo enhancement, and lateral shadowing [5]. In relation to the halo features, it has been reported that the presence of halo on grayscale US is detected in 67% in all epidermal cyst [10], while the presence of a halo represents 61.5% in unruptured type [4]. They suggested that a higher frequency of the absence of a halo was statistically recognized in the ruptured cysts than in the unruptured ones [4]. The hypoechoic halo of epidermal cyst might be consistent with the more complete walls of cysts composed of keratinizing stratified squamous epithelium. Whereas ruptured cyst represents lobulated shape, a poorly defined boundary, absence of a halo [4]. Pericystic change has been also detected in ruptured type [11]. Figure 1a shows pseudotestis pattern with filiform anechoic areas, echogenic reflectors and hypoechoic rim on gray-scale US, which is pathologically confirmed in the right mandibular location.
Color Doppler Utrasonograpic Appearances
Unruptured type shows usually no substantial blood flow, while pericystic changes are demonstrated in ruptured type on grayscale US and color Doppler US shows pericystic changes and/or peripheral vascularity [11,12]. A few peripheral blood flow signals were depicted on color Doppler US (Figure 1b).
Real-time Tissue Elastography Appearances
Real-time sonoelastography is an ultrasound-based technique using the property that the tissue strain due to compression is lower in hardness tissues [6]. RTE is widely used for diagnosis of breast [7], thyroid [8] and testis lesions [9] on tissue elasticity. Typically, red is used to represent softer tissues, blue represents harder tissues, and yellow or green shows intermediate elasticity [28]. While shearwave elastography (SWE) namely termed dynamic elastography, is based on the measurement of the propagation velocity distribution of the directional shear wave, produced by an ultrasound pulse [28]. It is sometimes difficult to distinguish an epidermal cyst from other benign skin tumors, such as lipoma, ganglia, pilomatricoma and dermatofibroma. Some studies have been reported on RTE [5,13-15] and on SWE [16]. Lee et al. concluded that the stain ratios of lipoma, ganglia, were statistically different from epidermal inclusion cysts but there was no statistically difference between epidermal inclusion cyst and pilomatoricomas [14]. Park et al. described that the strain elastography score was classified into four types.
Their data recognized variable elasticity of epidermal cyst. They indicated that superficial epidermoid tumor shows a softer nature than dose malignant tumor; however, it does not have a different SE pattern from other benign tumors [15]. The author previously reported the nonpseudotestis type of epidermal cyst which was pathologically confirmed in the plantar location [13]. Image features on RTE showed more green than blue, suggesting relatively soft nature [13]. Nodule demonstrated more green than blue, showing relatively soft nature, while the peripheral rim showed green to red color consistent with soft nature, suggesting no fibrotic condition (Figure 1c). Our data indicates that epidermal cyst is relatively soft nature, but it seems to be harder than lipoma. With respect to the ruptured study, it has been studied that R value inside the cyst (Rinside), R value outside the cyst (Routside) and Rinside/Routside ratio, which shows the ratio of the elasticity inside and outside the cyst, were examined on sonoelastography [5]. They concluded that RTE is able to detect differences in tissue elasticity between ruptured and unruptured epidermal cysts [5]. On SEW, it is reported that epidermal cyst statistically showed a greater median shear modulus than ganglion cysts and lipomatous tumors [16]. Meanwhile, it has been reported that neurogenic tumors or neuromas, dermoid cysts, and metastatic tumors were considered as high stiffness, namely low elasticity, while lipoma, lymphatic and/or venous maiformations, and cystic tumors show low stiffness, so-called high elasticity [28,29].
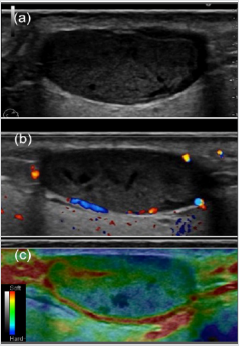
Figure 1: Pseudotestis type of epidermal cyst on gray scale US pathologically diagnosed in the right mandibular location in a 41-year-old man.
a) On gray-scale US shows pseudotestis pattern with filiform anechoic areas, echogenic reflectors and hypoechoic rim.
b) A few peripheral blood flow signals on rim are depicted on color Doppler US.
c) Epidermal cyst shows more green than blue, peripheral rim represents green to red color consistent with soft nature, suggesting without fibrosis condition on Real-Time Tissue Elastography.
Peripheral Rim Appearances
The rim on gray-sale US showed a sharply defined hypoechoic or hyperechoic rim surrounding the epidermal cyst. Kim et al reported that peripheral low echoic rim, consistent with the capsule was detected in 67% on gray-scale US [10]. Yuan et al. have statistically emphasized a higher frequency of the absence of a halo in the ruptured cysts than in unruptured cysts [4]. The hypoechoic halo of ruptured and unruptured epidermal cysts might represent the more complete walls of cysts composed of keratinizing stratified squamous epithelium [4,11,26]. It has been suggested that if the fragmented wall of a ruptured epidermal cyst is involved with an inflammatory reaction or granulation tissue, the sharpness and continuity of the walls would pathologically disappear, and the halos on gray-scale US would be absent [4]. With respect to peripheral rim features on RTE, there have not been reported bibliographically. Soft nature of rim appearance, showing without fibrosis may be consistent with unruptured type. Rim feature on RTE may contribute to determine the accurate diagnosis in differentiation unruptured type from ruptured type.
TRE procedure is evaluated using elasticity state not only in malignancy grade but also in fibrosis condition. Thin and smooth rim with soft nature, having high elasticity on RTE indicate no fibrosis, reflecting the possibility of the unruptured condition. In relation to MRI findings, it is reported that epidermal cyst shows high signal intensity on T2 and all peripheral rim enhancement [10]. Thin and smooth rim enhancement was shown in unruptured type, while the thick and irregular rim enhancement was demonstrated in ruptured type [30]. They also have noted that most ruptured epidermal cyst contained septa and showed thick and irregular rim enhancement and fuzzy adjacent soft-tissue enhancement [30]. Fisher et al. have suggested that the rim enhancement might be due to fibrosis and foreign body reaction around the cyst wall remnants and keratinous material [31]. Axial T2-weighted image shows hyperintense mass which was pathologically diagnosed as epidermal cyst in the right mandibular location (Figure 2a). Thin and smooth rim enhancement was also shown on contrastenhanced T1-weighted image, suggesting unruptured type of epidermal cyst (Figure 2b).
Pathological Appearances
If epidermal cyst rupture, suppuration, foreign body granulomatous reaction, and granulation tissue can be recognized [32]. It has been reported that the contents of the cysts in the ruptured cyst included more abscess, parakeratotic cells, red blood cells, giant cells and pilomatoricoma-like cells than in the unruptured type [33]. With respect to cystic wall, hyperplasia, hypergranulosis, microabscess, parakeratosis, necrotic change, verrucous changes and exocytosis, which were revealed more in the ruptured type than in the unruptured one [33] Figure 2c showed cystic lesion lined by stratified squamous epithelium with variable amounts of keratinous debris and packed keratin lamellae. Cystic lesion with a stratified squamous epithelial lining, keratinous debris, multinucleated giant cells, and inflammatory reactions were also observed (Figure 2d).
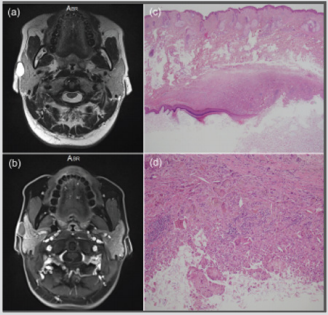
Figure 2: Pseudotestis type of epidermal cyst on gray-scale US pathologically diagnosed in the right mandibular location in a 41-year-old man.
a) Axial T2-weighted image shows hyperintense mass.
b) Thin and smooth rim enhancement is shown on contrast-enhanced T1-weighted image.
c) Cystic lesion lined by stratified squamous epithelium with variable amounts of keratinous debris and packed keratin lamellae are noted (hematoxylin-eosin, original magnification x10).
d) Cystic lesion with a stratified squamous epithelial lining, keratinous debris, multinucleated giant cells, and inflammatory reactions are shown (hematoxylin-eosin, original magnification x50).
It is suggested that epidermal cyst is relatively soft nature, but it is plausible that epidermal cyst is harder nature than lipoma on RTE. In relation to the ruptured state, it may be helpful finding that ruptured type is softer nature than unrptured type. Peripheral rim on gray-scale US statistically seems to be detectable in unruptured type than in ruptured epidermal cyst. Thin and smooth rim on enhanced MRI and soft nature on RTE, having high elasticity, indicate no fibrosis, reflecting the possibility of the unruptured condition. In addition to the enhanced MRI, evaluation of the elasticity on RTE in peripheral rim is useful for correct diagnosis in differentiating ruptured from unruptured type.
Conclusion
a) The author suggests epidermal cyst is relatively soft nature, but it is plausible that epidermal cyst is harder nature than lipoma on Real-Time Tissue Elastography.
b) Thin and smooth rim on enhanced MRI with soft nature on Real-Time tissue Elastograhy, having high elasticity, indicate without fibrosis, reflecting the possibility of the unruptured condition.
c) The author will suggest that thin and smooth on enhanced MRI and soft nature on Real-Time Tissue Elastography in peripheral rim features contribute accurate diagnosis of unruptured epidermal cyst.
Acknowledgement
The author appreciates Dr. Akira Fujioka, Dr. Minoru Oishi, and Dr. Ken Hayashi.
More BJSTR Articles: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.