Assessment of Respiratory Symptoms among Woodworkers in Jimma Town, Southwest Ethiopia, A Comparative Cross-Sectional Study
Introduction
Jimma is one of the oldest cities of Ethiopia, known as the ever green, forestry, 13 month of raining, coffee land and endemic with wood and wood products [1]. Many scholars also argue that Jimma was claimed as the home of respiratory disorders especially asthma [2]. The present study hypothesis that the unique and endemic of the town with wood and wood products exposes woodworkers to different respiratory disorders which manifested with respiratory sign and symptoms as occupational hazard. Exposure to wood dust is responsible for development of varies respiratory diseases as occupation hazard and affecting about two million workers worldwide [3-6]. Dusts from the wood and its different components enters into respiratory systems via inhalation to cause respiratory disorders by sensitizing and irritating mucous membrane of airways which are manifested by different sign and symptoms among exposed wood workers [7-14]. A meta- analysis study conducted in Great Britain has shown exposure to woodwork was associated with significantly increased risk of respiratory symptoms and asthma among furniture and wood processing [15].
The other study conducted in Asian countries revealed that wood dust is more prone to cause irritant respiratory symptoms and a potent cause of chronic respiratory diseases among wood workers [9]. Despite there is no study conducted on the interested area in the setting and as well as in the country, there are different studies conducted among woodworkers to evaluate the magnitude of respiratory symptoms globally [3,5,8,11-14,16-36]. Previous study conducted in the setting among woodworkers reported higher magnitude of respiratory disorders than the control group [37] and also study done among cobblestone road paving workers revealed the significant higher odds of respiratory symptoms, (dry cough (p < 0.05), cough (p < 0.01) and sore throat (p< 0.001)) compared to the reference group [38]. Study conducted among street sweepers in Addis Ababa showed the high prevalence respiratory symptoms [39]. Thus, the present study was aimed to assess respiratory symptoms among wood workers in Jimma town by taking reference group.
Materials and Method
Study Area and Period
The study was conducted in Jimma town, located in the Oromia region, about 354 km distance to southwest direction, from the capital city of the country and Oromia, Finfinne. The town has 17 kebeles with a total population of 159,009 of whom 80,897 were males. The town has an altitude of 1750-2000 m above sea level with a temperature range of 20-30oC and average annual rainfall of 800-2500mm3. According to Jimma town entrepreneur and food security agency of 2017/2018 report, there are 300 small-scale wood processing industries in the town involving 1012 male and 548 female woodworkers. The data was collected from April 5 to May 3, 2018 G.C among sampled wood workers and non-exposed group (shopkeepers) for comparison by employing comparative cross-sectional study design.
Selection Criteria
The woodworkers as exposed group with one year and above experience and non-exposed group (shopkeepers) who had never worked in woodwork or other wood related industry were recruited in matching with year of service, age, sex and BMI. All individuals of both groups (exposed and non-exposed) with history of pulmonary tuberculosis, heart failure, common cold, history of smoking, any acute illness was excluded from the study.
Sample Size Determination
The sample size was determined by using analytical study sample size calculation formula by taking two-sided confidence level of 95%, a power of 80% with a double proportion formula.
Where: n = sample size required in each group
Z a/2 = critical value at 95% confidence level of certainty (1.96) (a constant).
β: This depends on power, (the probability that if the two proportions differ the test will produce a significant difference) for 80% this is .84
P1=Prevalence of symptoms among exposed group/cases
P2= Prevalence of symptoms among non -exposed controls
p = average percentage between two groups= (p1+p2)/2
q = 1−p
d = clinically meaningful difference between two groups (p1- p2)
r= ratio of exposed to non-exposed =1 because of equal number of exposed to non-exposed group.
Based on the previous study conducted in Cameroon by Francis NDE et al with the magnitude of respiratory symptoms among woodworkers (cough 34.5% among exposed group and 6.6% among non- exposed group) was used for sample calculation [16].
n (each group) = [(2)x(.21) x(.79) x(1.96+.84)2]/(.345-.066)2= 33.4*2 (two groups)≈67. Due to multi -stage sampling technique the calculated sample size was multiplied by 2 (design effect) which equals to 134. By adding 5% of the non- response rate the total sample size was 140 for both exposed and non-exposed groups.
Sampling Technique
Multistage sampling technique was used to select the exposed study participants. First, five kebeles were selected by simple random sampling from the total 17 kebeles of the town. Then, by considering equal weight allocation of the sample to each selected kebeles; 14 small-scale wood work enterprises were selected by simple random sampling from the total 300 small-scale wood processing industries distributed in kebeles of the town. From each enterprise, one eligible respondent was selected by simple random sampling method. The comparison group of shopkeepers was selected by convenience sampling technique matching with age, sex, duration of service and body mass index to sampled woodworkers. (Figure 1).
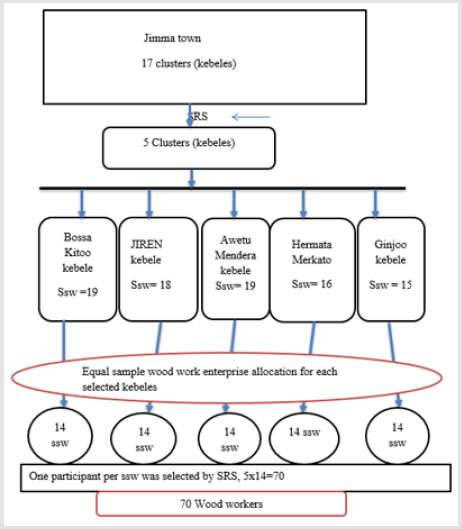
Figure 1: Schematic presentation of sampling procedure conducted to select study participants among woodworkers in Jimma town, southwest Ethiopia 2018 G.C.
(Source: Jimma town Entrepreneur & food security Agency, 2017/2018).
SRS=Simple Random Sampling, SSW=small scale woodwork industry
Data Analysis
Data was checked for completeness, entered into Epi-data version 1.7 and finally exported to SPSS version 20 for further analysis. Descriptive statistics were used to summarize the finding. Statistical analysis of the difference between proportions was done by the use of the chi-square test.
Ethical Consideration
Ethical clearance was obtained from the Institutional Review Board (IRB) of Jimma University, Institute of Health with specific number of 260/2018. Letter of cooperation was obtained from Jimma university postgraduate school to facilitate study. Oral and Written consent was obtained from participants before data collection. The objectives of the study were explained to each study participants. The information obtained in the study participants was handled confidentially and not disclose to third party.
Results
Socio- Demographic Characteristics
A total of 140 (70 woodworkers and 70 shopkeepers) were recruited in the study. The mean age of woodworkers and nonwoodworkers were 27.86 (SD±7.88) years and 26.49 years (SD ±5.378) respectively. The mean height and weight of woodworkers and non-woodworkers were 169.90 cm (SD± 6.084) vs 170.66 cm (SD± 5.941) and 59.89 Kg (SD ± 5.77) vs 59.99 Kg (SD ± 5.59) respectively. The mean service year duration of woodworkers and non-woodworkers was 7.20 ± 5.45and 7.45± 4.40 respectively with range between 1 to 22 years in both groups (Table 1).
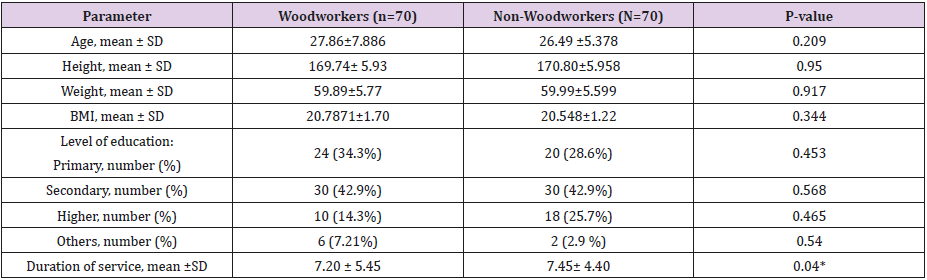
Table 1: Socio -demographic characteristics of woodworkers and reference population in Jimma town, Southwest Ethiopia, 2018 G.C.
P<.05 significant, BMI- body mass index, SD-standard deviation
*- Significant p-value for prevalence of respiratory Symptoms
Prevalence of Respiratory Symptoms
The prevalence of the respiratory symptoms in the last 12 months was higher among woodworkers when compared to nonwoodworkers. The prevalence of dry cough, cough with phlegm expectoration, chest pain, breathlessness, and wheeze with 95% confidence interval were 41.4% (31.4 - 51.7), 34.3% (25.5 - 48.6), 32.9% (22.6 - 47.1), 21.4% (9.7 - 29.1), and 12.9 % (5.2 - 22.9) for exposed study participants respectively and the prevalence of phlegm expectoration, dry cough, chest pain, breathlessness, and wheeze for non- exposed group with 95% confidence interval were 14.3% (5.7 - 23.1), 10% (2.6 - 17.4), 17.1% (10 - 28.2), 14.3% (5.7 - 23.7) and 8.6% (3.5 - 17.1) respectively. Moreover, all respiratory symptoms except breathlessness and wheezing showed statistically significant differences between woodworkers and non-woodworkers. Woodworkers were 6.36 times more likely to develop dry cough, 2.94 times more likely to phlegm production, 2.36 times more likely to have chest pain, 1.64 more likely to develop breathlessness and 1.57 times more likely to develop wheezing than non-woodworkers.(Table 2).
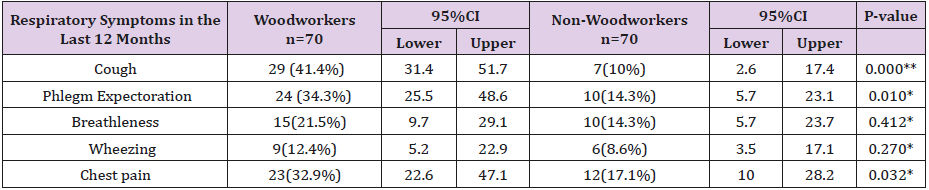
Table 2: The prevalence of respiratory symptoms in the last 12 months in woodworkers and non-woodworkers in Jimma town, Southwest Ethiopia, 2018.
Statically significant (p<.05), **p<.0001
*Tested by chi-square test
Discussion
The finding of the present study revealed that exposure of wood dust among the woodworkers resulted in higher prevalence of respiratory symptoms compared to non-woodworkers. There is statistically significant difference discriminated among the groups in cough (41.4% vs. 10%), phlegm expectoration (34.3% vs.14.3%), chest pain (32.9% vs. 17.1%). But the prevalence of breathlessness and wheeze among woodworkers were higher than non-woodworkers but didn’t reach statistical significant difference between groups. The higher prevalence of respiratory symptoms among woodworkers could be air pollution in the working environment due to wood dust resulting in activation and infiltration of inflammatory cells (T cells, mast cells, basophils, eosinophil’s, neutrophils, and/or macrophages) in the respiratory system and allergic sensitization that could facilitate the development of allergic alveolitis, hyper-responsiveness of the air ways, irritation of cough receptors, hypertrophy of smooth muscle cells due to recurrent hyper-responsive bronchial constriction and hyperplasia of goblet cells that leads to development different respiratory symptoms [41-43].
The present finding was comparable to study done by Francis NDE et al who revealed higher prevalence of respiratory symptom among woodworkers than non-woodworkers with magnitude of dry cough 34.5% vs. 6.6% and phlegm expectoration 3.1 % vs. 0.8% respectively with statistically significant difference [16]. Another study conducted in Republic of Macedonia by Dragana Bislimovska et al also supported the present finding as reported higher prevalence of respiratory symptoms among woodworkers than non-woodworkers with magnitude of cough (29.7% vs. 13.5%), phlegm (15.2% vs. 5.4% ), shortness of breath (10.8% vs. 8.1%), chest pain (13.5% vs. 10.8% ) respectively [26]. The present study was also in harmony with study of Tobin EA et al who reported the higher prevalence of respiratory symptoms among the exposed study group [cough 46.7%, phlegm expectoration 50.2%, wheeze 5.3%, chest tightness 10.1%, chest pain 5.7% and breathlessness 7.5% ] than the comparison group [24]. The present finding was also in agreement with results of other studies [25,36,44,45].
Study Limitation
The respiratory symptoms were assessed based on study participant health history; so, it might be prone to recall bias. This study didn’t measure concentration of dust between woodwork and shopkeepers working environment. The present study didn’t include both sexes because of unavailability of female woodworkers.
Conclusion
The prevalence of respiratory symptoms among wood workers was higher than non-woodworkers. Moreover, all respiratory symptoms except breathlessness and wheezing showed statistically significant differences between woodworkers and nonwoodworkers.
For more Articles: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.