Implications for the Inclusion of Echo Intensity for Athlete Monitoring: A Mini Review
Introduction
Sport practitioners (i.e., sport scientists, strength and conditioning coaches, sport coaches, and sports medicine staff) must implement appropriately planned annual training regimens, recovery strategies, and use both accepted and novel athlete monitoring protocols to continually progress athletic performance. Ultrasound measurements have been used extensively throughout the literature as a reliable and valid method for examining muscle structure and muscular adaptations as a result of resistance training [1]. Although this noninvasive method is comparable to other measurement methods such as magnetic resonance imaging [2], ultrasonography is the most practical, resourceful, and time efficient procedure for sport practitioners to implement regarding athlete monitoring. Ultrasound is most commonly used for measuring muscle quantity (i.e., muscle cross-sectional area [CSA]) [3]; however, when assessing only the size of the muscle, ultrasound instrumentation has limitations and cannot account for muscular hydration, glycogen content, triglyceride accrual, inflammation or edema (i.e., muscle swelling). More recently, echo intensity (EI) has been used to determine muscle quality (i.e., intramuscular fibrous and adipose tissue, noncontractile elements) and may give insight into the intramuscular and intermuscular cellular environments [4]. Therefore, monitoring skeletal muscle adaptations in relation to both muscle quantity and quality as a result of resistance training should be considered a mainstay for long-term athlete development [5]. Thus, the purpose of this mini review is to highlight the usefulness of incorporating EI as a sub-analysis of muscle CSA assessments for sport practitioners who currently implement ultrasound instrumentation as part of an ongoing athlete monitoring program.
Most Common Usages for Ultrasound
For the general population, ultrasound has been used most commonly to assess injuries, mortality, disease, muscle quantity and muscle quality as it relates to strength and power [6-8]. For example, previous studies have shown that muscle quality of skeletal muscle was indicative of overall strength and power in healthy elderly individuals [9]. Additionally, positive correlations have been observed between torque per unit of muscle mass and cardiovascular parameters (r=0.52 to r=0.60; P < 0.001) giving insight into the potential use to assess neuromuscular and cardiovascular performance. Echo intensity has been shown to independently contribute to muscle strength in both middle-aged and elderly persons and has shown the same contribution in the athletic population [10].
Contemporaneously, sport practitioners have used similar methods to specifically access muscle quantity to determine the effectiveness of periodization and programming as well as an athlete’s potential performance capability (i.e., talent identification) [11,12]. For example, in a squadron of track and field athletes ranging from throwers to distance runners, despite their high amount of body fat, the throwers ability to express strength and power was associated with the lowest EI values (63.4±5.2 au) compared to athletes of other disciplines. Hirsch et al. [13] showed that when evaluating muscle characteristics in addition to body composition assessments EI would be valuable for detecting performance improvements, preventing injuries, and assessing potential health risks. Considering that muscle CSA has been shown to be indicative of performance regarding overall strength, power output, rate of force development, and jumping ability, EI seems to be a sufficient sub-analysis for sport practitioners to assess training adaptations and recovery across a broader spectrum (Figure 1).
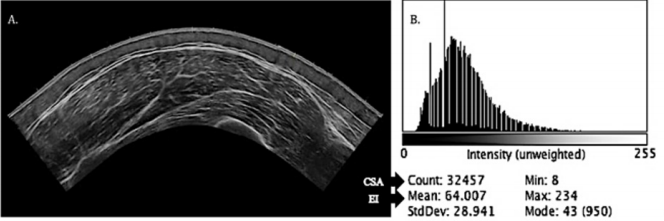
Figure 1: Ultrasound vastus lateralis imaging and grayscale analysis software histogram output.
Note: Image A is a direct output from the ultrasound machine. Image B is the computer aided grayscale analysis software with the histogram output. CSA= muscle cross-sectional area; EI= echo intensity. Count corresponds to muscle CSA: 32457=32.457 cm2 . Mean corresponds to EI value: 64au.
Implementing the Sub-Analysis
By extracting the image produced from an ultrasound collection period, EI may be used to quantify the quality of the muscle using grayscale analysis that analyzes the pixel count which provides a score ranging from 0 to 256 au (0=black and 256=white) [8] (Figure 1). Across the grayscale spectrum, individuals with high muscle quality tends to be hypoechoic or closer to 0 [14] whereas those with poor muscle quality tend to be hyperechoic or closer to 256 [15]. This information is visually presented on the output system provided by a histogram display. A hypoechoic EI output would be associated with a high amount of lean body mass, ideal body composition, low inflammation and low edema or, acutely, an athlete in a recovered state with the histogram peaking towards the left [16]. A hyperechoic EI output would be associated with high-fat mass and poor body composition or possibly an acute physiological disturbance such as inflammation, increased creatine kinase from muscle breakdown, or edema (i.e., histogram peaking towards the right) [17].
Athlete Monitoring
Considering that muscle CSA is typically already analyzed for ultrasound imaging, sport practitioners may use a computerized grayscale analysis software to gather the desired information that includes the CSA and EI value for a given image simultaneously (Figure 1). Echo intensity may be used longitudinally for longterm athlete monitoring (Figure 2) or for more frequent testing to observe an athlete’s acute training responses (Figure 3). This assessment would be most useful to compare muscle characteristic changes during preparatory training periods to competition preparation training periods [18]. Sport practitioners who use true periodized training models (i.e., annual planning) often incorporate athlete monitoring testing sessions throughout a given year [19]. Most frequently, these testing sessions occur at the beginning, in the middle, and at the end of an annual training year [20]. Sport practitioners may use an image transparency function for successive CSA and EI outputs to determine positive or negative shifts from the output diagram (e.g., Figure 2 shows an improvement in muscle quality). It is important to note, that ultrasound images are typically collected after 24-48 hours of rest or during active recovery periods [21] and should be collected in accordance with previously published methodology to acquire accurate results for both CSA and EI analyses (Figure 2).
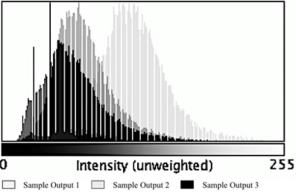
Figure 2: Echo intensity for longitudinal athlete monitoring.
Note: Sample output 3 represents a baseline measurement. Sample output 2 represents a mid-training cycle measurement. Sample output 1 represents a final measurement post-training cycle.
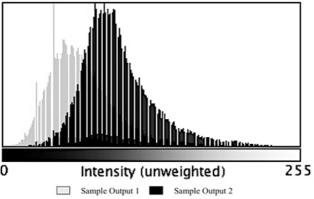
Figure 3: Echo intensity for acute athlete monitoring.
Note: Sample output 1 represents training session 1. Sample output 2 represents training session 2 which may take place 1 week later.
From an acute perspective, the same image transparency function may be used from microcycle to microcycle (i.e., week to week) or bi-weekly to assess more frequent muscle alterations and adaptations [22]. In this case, muscle quantity outputs may be analyzed as a false-positive due to acute muscle swelling. Recently, Damas et al. [9] showed that the ratio of EI to muscle thickness at week three of a resistance training program was significantly altered relative to baseline due to edema rather than an actual improvement in muscle quantity or quality. Therefore, an acute change in the peak of the histogram shifting right may give insight into possible triglyceride accrual, water and glycogen retention, or overall muscle damage [23]. Sport practitioners may use this information to guide the training process to get a better understanding of how the athlete responds to specific training phases (i.e., accumulation, transmutation, realization) in relation to the total work accomplished and the time it takes for the local muscle to fully recover [24]. Acute hyperechoic values over a 4-week mesocycle have been shown to mask the ability to produce force for maximal 1-repetition-maximum strength [25]. Therefore, acute EI values may guide sport practitioners’ decisions leading into a competition to ensure that athletes are adequately recovered to express peak levels of performance on the day of competition (Figure 3).
Conclusion
The evidence presented on this topic provides insight into the rationale behind incorporating EI into an ongoing athlete monitoring program, particularly for sport practitioners who already use ultrasound measurements. Although it is not as common, multisite ultrasound collection for upper and lower extremities (e.g., triceps and vastus lateralis) may be warranted to determine an upper-tolower extremity EI ratio to understand whole body muscle quality [26]. This information may aid in guiding the training process further in the case that if lower extremity acute EI is altered significantly, upper body training may be implemented and emphasized accordingly. Further, if an athlete’s muscle quantity improves but muscle quality does not change over the course of an annual training year, the sport practitioner should consider adjusting the training protocol to elicit the desired adaptions. However, it should be noted that further EI studies need to be carried out to ensure that EI outputs correspond to actual physiological changes taking place within muscle tissue to negate more expensive, costly procedures such as muscle biopsies or blood draws [27]. We advocate for sport practitioners to assess large muscles that are easily accessible and often examined throughout the literature (e.g., vastus lateralis) so that data-driven decisions may be made regarding training or practices changes. Incorporating EI does not require additional time for the athlete monitoring process to be carried out nor further analysis procedures; EI provides an additional variable to account for both intramuscular and intermuscular muscular environments in relation to overall recovery and adaption that, in turn, improves performance.
For more Articles on : https://biomedres01.blogspot.com/

No comments:
Post a Comment
Note: Only a member of this blog may post a comment.