The Incidence of Malaria in Human Population of Shergarh District Mardan Pakistan
Introduction
Malaria being one of the most infectious diseases is caused by
unicellular parasites belong to Plasmodium genus. There are five
malaria causing species of this genus including Plasmodium vivax,
plasmodium falciparum, plasmodium ovale, plasmodium malariae
and plasmodium knowelsi [1,2]. These species show variation
in their morphology and drug resistance pattern, geographic
distribution and their mode of pathologic process [2]. In 2016, an
estimated number of 216 million cases of malarial infection have
occurred worldwide leading to an estimated 445,000 deaths
[3]. P. falciparum is taken into account the foremost fatal among
all species, and accounts for most of the deaths due to malaria
infection worldwide [4]. This infection is transmitted by a bite of
infected Anopheles, female mosquito specie that introduces the
plasmodium in its secretion into human blood system and leading
to a number of symptoms including headache and fever, and in
severe cases leading to death [5]. The infection is often diagnosed
by the microscopic examination of blood using blood films or
with antigen-based fast diagnostic tests. Molecular techniques
are employed to diagnose the infection; however, these molecular
strategies are not widely used because of their quality and
cost [6]. Malaria infection is widely occurred in 109 countries
mostly located in the tropics and sub-tropics [7].
In Africa, Papua and Haiti, P. falciparum is the the predominant species, where as P. vivax infection is endemic in the regions of Central and South America, North Africa, Near East and Indian landmass [8]. In Asia, particularly in Pakistan and Afghanistan, malaria continues to be a major public health issue with current transmission of each P. falciparum and P. vivax [9,10]. Pakistan, India, Ethiopia and Dutch East Indies contribute the 81% mortality due malaria infection [11]. Around 95 million people in Pakistan live in areas with high prevalence of malaria infection [12]. It was almost completely eradicated in sixties however the abrupt rise of malaria infection occurred in Seventies. Within the last 20 years, rise in malarial cases has been attributed to prolonged monsoon season and floods that affected twenty million individuals in over sixty districts [13]. P. vivax contributed 65% of cases while the remaining 35% cases were caused due to P. falciparum infection, in Pakistan. In spite of malaria control and vector management programs in Pakistan, 5 million new cases of malaria and a substantial number of deaths are reported. Approximately 37% of cases have been reported in the areas of Pakistan located near Afghanistan border and other neighbor countries [14]. This study was designed to report the incidence of malaria infection along with the distribution of prevalent plasmodium species in Shergarh; a rural area of district Mardan Pakistan.
Study Area
This study was carried out at Rural Health Center (RHC)
Shergarh Mardan. Shergarh is one of the populated towns of Mardan
is situated on the main highway between Mardan and Swat. It is
about 15 kilometers from the Malakand Mountains to the north, 12
km from Lund Khwar and 27 km from Mardan to the south.
Study Population
Subjects for this cross-sectional study were the febrile patients attending Rural Health Center (RHC) hospital Shergarh, Mardan. Subjects were divided into three groups on the basis of their ages i.e. group A: 1-15 years, group B: 16-30 years and group C. 31-45 years. The study consisted of 2830 blood samples from 1560 male and 1270 female subjects aged 1-45 years during August 2015 to July 2016 inhabitants of Shergarh District Mardan Khyber Pakhtunkhwa Pakistan.
Sample Collection
Some necessary information was collected from subjects regarding sex, age, residence, parent’s occupation, general health condition, past history of malarial infection, surrounding conditions of their home, and presence or absence of domestic animals. Blood samples were collected from subjects and labeled properly.
Preparation of Thick and Thin Blood Smears
Thick and thin smear were prepared on the same slide from the finger pricked blood samples of all subjects under study. Fixation of the thin smear was done with methyl alcohol. Blood films were stained with 10% Giemsa stain. The screening was done under microscope 100X objective with oil immersion. All slides were cross checked by senior microscopist in RHC (Shergarh) Mardan.
Results
During current study blood samples of 2830 subjects with fibril fever were investigated for malaria infection. Out of 2830 samples, 228 samples were found positive for malaria showing 8.05% incidence of malaria infection in the area. In positive samples, 122 (53.50%) were found as males while106 (46.5%) were females. The highest ratio of positive cases was observed in male subjects in age group C as 65(28.50 %) followed by age group B as 42 (18.42%) and lowest in age group A as 15(6.57%) (Figure 1). In female the highest ratio was reported in age group C that is 56 (24.56%) followed by age group B as 28 (12.28%) and lowest in age group A as 22(9.64%) cases. Among the infection causing species, P. vivax species was found to be responsible for all the infections in the area reported in this study while no other species including P. falciparum has been founded (Table 1)(Figure 2). Month wise prevalence of plasmodium parasite was found the highest in September as 49 (21.49%) while the lowest rate was found in months of January and February as only 1 (0.43%) followed by month of March and July as 4 (1.75%), and 5(2.19%) respectively (Figure 3). Among the studied samples of 1270 female subjects, 106 were found positive. The mean prevalence of malaria was high in non-pregnant women as compared to pregnant women. In pregnant women the prevalence was very low that is 8 (7.54%) while in non-pregnant it was recorded as 98 (92.45%) infected subjects (Figure 4).
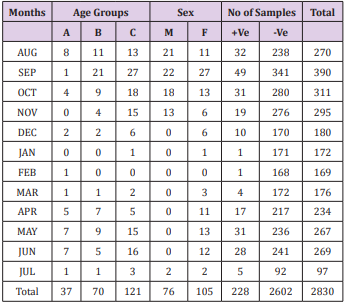
Table 1: Over all prevalence of plasmodium species.
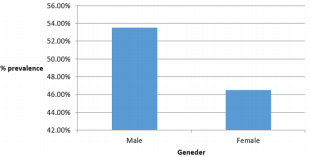
Figure 1: Gender wise prevalence of malaria in positive samples in RHC Shergarh Mardan.
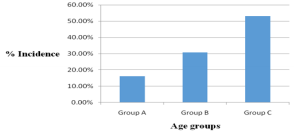
Figure 2: Age wise prevalence of malaria in Shergarh Mardan.
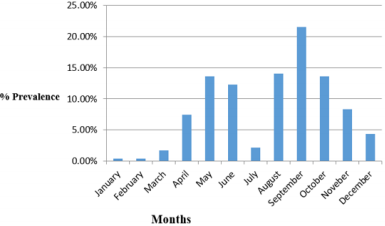
Figure 3: Month wise prevalence of malaria in RHC (Shergarh) Mardan.
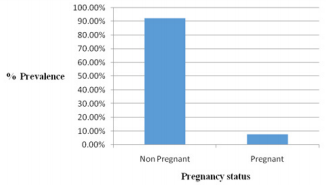
Figure 4: Malaria infection with respect to pregnancy status.
Discussion
Malaria is considered to be one amongst the leading causes
of morbidity and mortality worldwide, particularly in tropical
and sub tropical areas of the world. The infecting rate of malaria
infection in Pakistani community is concerning one million each
year. Malaria is the second most typical illness in West
Pakistan that accounts for 16.5% disease burden rate
across the country. Nearly 0.3 million microscopic examined
confirmed cases were reportable in 2011. More than 80% cases
of malaria were contributed by P. vivax and the remaining by
P. falciparum [15]. The present study is compared with Kashif
Rahim that was conducted in BHU Gala Der District Mardan in
which the prevalence rate was 13.9%. The sample size of that
study was 782 while the simple size in present study is 2830.
In present study the prevalence rate is low as compared to
other study that was conducted in District Mardan. It is difficult
to predict trends of malaria incidence in Pakistan, because of
fluctuation of malaria confirmed cases on yearly basis [16].
Another study conducted in Lal Qila, Lower Dir, revealed 29% malaria incidence [17] while 27% in Bannu [18] and about 33% in Barkhan and Kohlu districts of Balochistan have also been reported [19]. A study conducted in Abbottabad reported 7% malaria cases [20], while Buner district had 7% prevalence [21]. A study conducted on clinical isolates from Sindh province reported about 3% malaria endemic [21]. Within population variation in prevalence and distribution of plasmodium species might exist, unfortunately, there are no simple methodological explanations for this variability. Variation in malaria prevalence reflects the different dynamic of malaria transmission among different areas of Pakistan [22]. Similarly, a report from Dera Ismail Khan, revealed 95% of malaria cases were of P. vivax, [23] another study reported 96% P. vivax cases from Manshera [24], 82% P. vivax cases in Quetta [25] and 72% cases in Jacobabad [26]. A comprehensive higher population survey on malarial isolates from all over Pakistan reported P. vivax predominance by 76% [27].
The doable reason of high infection is that relapses overtimes occurred in P. vivax not in P. falciparum. The second reason is that P. vivax is usually gift in tropical and climatic zone areas [28]. This study shows that there was a considerable connection between malaria infection and gender in the study area as a higher infection rate was observed in males than females. It has been suggested for the disproportionate cases of malaria in male patients might be due to increased contact because males are more expected to work outside furthermore males not be as well covered as females which might be the possible reason for infected Anopheles bites. The malarial infections may also be associated with some degree of complicated sign and symptoms included prostration, any impairment of consciousness, convulsions or any manifestation of shock, decreased urinary output, respiratory distress or abnormal bleeding should be treated with parenteral rather than oral drugs [29].
Conclusion
This study showed that the prevalence rate of malaria
infection is comparatively more in male population with age
between 30-45 years. P. vivax is the most prevalent species in
the study area. The finding of this study will help in updating
the epidemiological profile of malaria in the study area and
other surrounding areas with same ecological conditions in
Khyber Pakhtunkhwa. Awareness of population and extending
better health facilities will help in control of malarial infection
in rural areas of Pakistan.
Acknowledgment
This study was supported by Higher Education Commission
(HEC) of Pakistan under NRPU program project No. NRPU-3474.
Introduction
Malaria being one of the most infectious diseases is caused by unicellular parasites belong to Plasmodium genus. There are five malaria causing species of this genus including Plasmodium vivax, plasmodium falciparum, plasmodium ovale, plasmodium malariae and plasmodium knowelsi [1,2]. These species show variation in their morphology and drug resistance pattern, geographic distribution and their mode of pathologic process [2]. In 2016, an estimated number of 216 million cases of malarial infection have occurred worldwide leading to an estimated 445,000 deaths [3]. P. falciparum is taken into account the foremost fatal among all species, and accounts for most of the deaths due to malaria infection worldwide [4]. This infection is transmitted by a bite of infected Anopheles, female mosquito specie that introduces the plasmodium in its secretion into human blood system and leading to a number of symptoms including headache and fever, and in severe cases leading to death [5]. The infection is often diagnosed by the microscopic examination of blood using blood films or with antigen-based fast diagnostic tests. Molecular techniques are employed to diagnose the infection; however, these molecular strategies are not widely used because of their quality and cost [6]. Malaria infection is widely occurred in 109 countries mostly located in the tropics and sub-tropics [7].
In Africa, Papua and Haiti, P. falciparum is the the predominant species, where as P. vivax infection is endemic in the regions of Central and South America, North Africa, Near East and Indian landmass [8]. In Asia, particularly in Pakistan and Afghanistan, malaria continues to be a major public health issue with current transmission of each P. falciparum and P. vivax [9,10]. Pakistan, India, Ethiopia and Dutch East Indies contribute the 81% mortality due malaria infection [11]. Around 95 million people in Pakistan live in areas with high prevalence of malaria infection [12]. It was almost completely eradicated in sixties however the abrupt rise of malaria infection occurred in Seventies. Within the last 20 years, rise in malarial cases has been attributed to prolonged monsoon season and floods that affected twenty million individuals in over sixty districts [13]. P. vivax contributed 65% of cases while the remaining 35% cases were caused due to P. falciparum infection, in Pakistan. In spite of malaria control and vector management programs in Pakistan, 5 million new cases of malaria and a substantial number of deaths are reported. Approximately 37% of cases have been reported in the areas of Pakistan located near Afghanistan border and other neighbor countries [14]. This study was designed to report the incidence of malaria infection along with the distribution of prevalent plasmodium species in Shergarh; a rural area of district Mardan Pakistan.
Study Area
This study was carried out at Rural Health Center (RHC) Shergarh Mardan. Shergarh is one of the populated towns of Mardan is situated on the main highway between Mardan and Swat. It is about 15 kilometers from the Malakand Mountains to the north, 12 km from Lund Khwar and 27 km from Mardan to the south.
Study Population
Subjects for this cross-sectional study were the febrile patients attending Rural Health Center (RHC) hospital Shergarh, Mardan. Subjects were divided into three groups on the basis of their ages i.e. group A: 1-15 years, group B: 16-30 years and group C. 31-45 years. The study consisted of 2830 blood samples from 1560 male and 1270 female subjects aged 1-45 years during August 2015 to July 2016 inhabitants of Shergarh District Mardan Khyber Pakhtunkhwa Pakistan.
Sample Collection
Some necessary information was collected from subjects regarding sex, age, residence, parent’s occupation, general health condition, past history of malarial infection, surrounding conditions of their home, and presence or absence of domestic animals. Blood samples were collected from subjects and labeled properly.
Preparation of Thick and Thin Blood Smears
Thick and thin smear were prepared on the same slide from the finger pricked blood samples of all subjects under study. Fixation of the thin smear was done with methyl alcohol. Blood films were stained with 10% Giemsa stain. The screening was done under microscope 100X objective with oil immersion. All slides were cross checked by senior microscopist in RHC (Shergarh) Mardan.
Results
During current study blood samples of 2830 subjects with fibril fever were investigated for malaria infection. Out of 2830 samples, 228 samples were found positive for malaria showing 8.05% incidence of malaria infection in the area. In positive samples, 122 (53.50%) were found as males while106 (46.5%) were females. The highest ratio of positive cases was observed in male subjects in age group C as 65(28.50 %) followed by age group B as 42 (18.42%) and lowest in age group A as 15(6.57%) (Figure 1). In female the highest ratio was reported in age group C that is 56 (24.56%) followed by age group B as 28 (12.28%) and lowest in age group A as 22(9.64%) cases. Among the infection causing species, P. vivax species was found to be responsible for all the infections in the area reported in this study while no other species including P. falciparum has been founded (Table 1)(Figure 2). Month wise prevalence of plasmodium parasite was found the highest in September as 49 (21.49%) while the lowest rate was found in months of January and February as only 1 (0.43%) followed by month of March and July as 4 (1.75%), and 5(2.19%) respectively (Figure 3). Among the studied samples of 1270 female subjects, 106 were found positive. The mean prevalence of malaria was high in non-pregnant women as compared to pregnant women. In pregnant women the prevalence was very low that is 8 (7.54%) while in non-pregnant it was recorded as 98 (92.45%) infected subjects (Figure 4).
Table 1: Over all prevalence of plasmodium species.
Figure 1: Gender wise prevalence of malaria in positive samples in RHC Shergarh Mardan.
Figure 2: Age wise prevalence of malaria in Shergarh Mardan.
Figure 3: Month wise prevalence of malaria in RHC (Shergarh) Mardan.
Figure 4: Malaria infection with respect to pregnancy status.
Discussion
Malaria is considered to be one amongst the leading causes of morbidity and mortality worldwide, particularly in tropical and sub tropical areas of the world. The infecting rate of malaria infection in Pakistani community is concerning one million each year. Malaria is the second most typical illness in West Pakistan that accounts for 16.5% disease burden rate across the country. Nearly 0.3 million microscopic examined confirmed cases were reportable in 2011. More than 80% cases of malaria were contributed by P. vivax and the remaining by P. falciparum [15]. The present study is compared with Kashif Rahim that was conducted in BHU Gala Der District Mardan in which the prevalence rate was 13.9%. The sample size of that study was 782 while the simple size in present study is 2830. In present study the prevalence rate is low as compared to other study that was conducted in District Mardan. It is difficult to predict trends of malaria incidence in Pakistan, because of fluctuation of malaria confirmed cases on yearly basis [16].
Another study conducted in Lal Qila, Lower Dir, revealed 29% malaria incidence [17] while 27% in Bannu [18] and about 33% in Barkhan and Kohlu districts of Balochistan have also been reported [19]. A study conducted in Abbottabad reported 7% malaria cases [20], while Buner district had 7% prevalence [21]. A study conducted on clinical isolates from Sindh province reported about 3% malaria endemic [21]. Within population variation in prevalence and distribution of plasmodium species might exist, unfortunately, there are no simple methodological explanations for this variability. Variation in malaria prevalence reflects the different dynamic of malaria transmission among different areas of Pakistan [22]. Similarly, a report from Dera Ismail Khan, revealed 95% of malaria cases were of P. vivax, [23] another study reported 96% P. vivax cases from Manshera [24], 82% P. vivax cases in Quetta [25] and 72% cases in Jacobabad [26]. A comprehensive higher population survey on malarial isolates from all over Pakistan reported P. vivax predominance by 76% [27].
The doable reason of high infection is that relapses overtimes occurred in P. vivax not in P. falciparum. The second reason is that P. vivax is usually gift in tropical and climatic zone areas [28]. This study shows that there was a considerable connection between malaria infection and gender in the study area as a higher infection rate was observed in males than females. It has been suggested for the disproportionate cases of malaria in male patients might be due to increased contact because males are more expected to work outside furthermore males not be as well covered as females which might be the possible reason for infected Anopheles bites. The malarial infections may also be associated with some degree of complicated sign and symptoms included prostration, any impairment of consciousness, convulsions or any manifestation of shock, decreased urinary output, respiratory distress or abnormal bleeding should be treated with parenteral rather than oral drugs [29].



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.