Comparative Efficacy of Tocotrienol and Tocopherol for their Anti Diabetic Effects
Introduction
The antioxidant and lipid soluble vitamin E have eight
compounds i.e α-, β-, γ-, δ-tocopherols and α-, β-, γ-, δ-tocotrienols.
The main source for the synthesis of these compounds is by
photosynthetic organisms like cyanobacteria, plants, algae, fungi,
sponges, corals, and tunicate. However, the foremost natural source
of both these compounds the oily fraction of nuts, oil seeds, almond
oil, olive oil, rapeseed oil, sunflower oil, linseed oil, corn oil, and
soybean oil. The source of tocotrienols, can be rice bran and palm
oil, barley, oats, wheat germ, maize, hazelnuts, and in annatto oil.
The highlighted sources for α-tocopherol and γ-tocopherol are
sesame, soybeans, and corn oil. Despite having similar structure and
antioxidant properties, these isoforms differ in their bioavailability
and metabolism [1]. The other difference is the amount of saturation
for hydrophobic tridecyl chain. Tocopherols have saturated phytyl tails
whereas tocotrienols have unsaturated isoprenoid side chain
with three double bonds [2].
With the advent of age, many pathologies used to come on
rise. The highlighted ones are the presence of hypertension, type
II diabetes, cardiovascular disorders, neurological deficit etc. These
all have strong relation with oxidative stress and inflammation.
Here comes the significance for using anti oxidative and antiinflammatory
to slow down the disease progression in view to
improve quality of life. The isoforms of vitamin E i.e tocotrienol is
notorious for both the above-mentioned properties. The reported
literature supports that tocotrienols inhibit pathways that are
involved in nuclear factor κB (NF-κB), signal transducers, activators
3 (STAT3) and cyclo-oxygenase 2 (COX-2). These all are the ones
which activate pathological inflammatory responses. Besides this
they are considered as the bioactive form of Vitamin E compared
to tocopherols. Hence comes the reason for its application in the
therapeutics [3].
Metabolic syndrome (MetS) also known as Syndrome X
and Insulin Resistance Syndrome. Metabolic syndrome (MetS)
refers to the presence of three or more amongst the five comorbidities:
obesity, systemic hypertension, prediabetes/diabetes,
insulin resistance, dyslipidemia with reduced HDL levels &
hypertriglyceridemia leading to increased risk of cardiovascular
disease. MetS involves chronic low-grade inflammation, with
elevated serum interleukin 6 (IL-6), IL-1b & CRP levels [4].
It is well known that diabetes mellitus is caused by a deficiency
in insulin secretion or by a low response of organs to the action of
insulin. Oxidative stress also leads to development & progression
of diabetes mellitus, since an exacerbated surge in production of
free radicals occurs simultaneously with repressed mechanisms of
antioxidant defenses resulting in cellular damage & increased lipid
peroxidation and ultimately the development of insulin resistance.
(Savelieff et al. 2020) In another study the beneficial effects of
T3s were observed for attenuation of inflammation and insulin
resistance especially in overweight or obese women [4].
Around the Globe, management of diabetes mellitus is always
a challenging task for the clinician. This is especially true to reduce
the emergence of early complications. Therefore, the researchers
are devoted to find the solution of this problem. In light of the
delicacy of matter, a randomized control trial (RCT) was carried out
in 2020, to assess a comparative efficacy of vitamins A, B, C, D&E
supplementation on the antioxidant status and glycemic index of
type 2 diabetes mellitus patients, The outcomes were measured
and compared by various lab tests in pre and post supplementation
period. The tests were malondialdehyde (MDA), changes in
total antioxidant capacity (TAC), augmentation of glutathione
peroxidase (GPx), enhance in superoxide dismutase enzyme (SOD),
and thiobarbituric acid reactive substances (TBARS) and glucose
levels. It was concluded that supplementation of vitamin E revealed
highest antioxidant efficacy [5].
Rationale
The process of aging is a non-modifiable risk factor predisposing to many pathologies. The highlighted one includes hypertension, type II diabetes, hypercholesterolemia, cardiovascular morbidities, and many other degenerative changes. The allopathic medicines impart great significance to address these issues. But besides beneficial effects, many side effects used to be there. Therefore, even with advancement in medical science, there is emergence for a necessity of herbal remedies or plant-based natural compounds. So alternative form of treatment search is being carried out Globally. The aim behind the current systematic review is to add up the knowledge for the efficacy of tocotreinol and tocopherol for managing a patient of diabetes with or without insulin resistance. This will be a step forward to reduce the sufferings and miseries of diabetic patients.
Methodology
This systematic review was carried out by following PRISMA protocol and PRISMA guidelines – 2019 [6]. Figure 1 shows the PRISMA flow diagram for the selected 05 (N) articles for current systematic review. Four steps were followed for final inclusion of 05(N) articles i.e identification, screening, eligibility and finally included ones. For identification, records of 86(n ) articles were identified by thorough search from various database. Sixty from PUBMED, 01(n) from Cochrane data base, 05(n) from Google scholar, 15 (n) from open Google search, 01(n) from PakMedinet, 01(n) from EMBASSE,01(n) from MEDLINE and zero form Cross Ref. Additional records identified through other sources by snowball effect from meta-analysis (n = 04), all from Pubmed , by snow ball method from a meta-analysis. Duplicate data was removed, and 15(n) articles were dropped. Screening was done for remaining 71(n) articles. Sixty-one articles were excluded due to various reasons and only 10(n) were found eligible. Amongst them 05(n) were excluded and only 05(N) were finally included for the current systematic review. The data was searched between the years 2021 to 2003. The details are shown in Figure I.
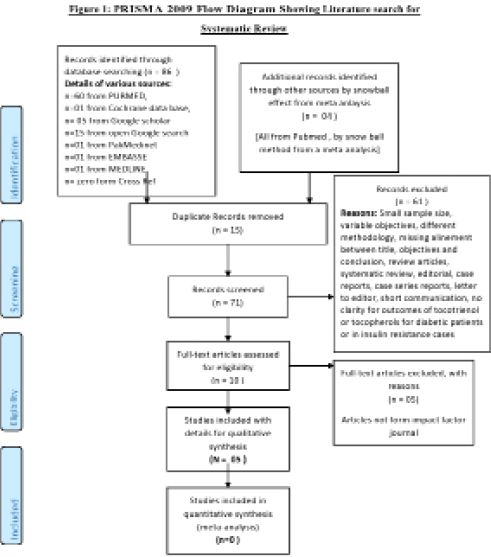
Figure 1: PRISMA 2009 Flow Diagram Showing Literature search for Systematic Review.
To ensure selection of authentic information certain MESH key
words/synonyms were used for searching the relevant literature
review. The selected key words were diabetes, vitamin E, tocotrienol,
tocopherol, effectiveness, insulin resistance, diabetic nephropathy,
diabetic neuropathy, diabetes complications. The inclusion criteria
of study were the studies related to the use of vitamin E, tocotrienol,
tocopherol, or their comparative efficacy in diabetic patients with
or without insulin resistance. Studies having details of either the
administration of any of four chemical forms of vitamin E i.e alpha-,
beta-, gamma-, and delta-tocopherol and alpha-, beta-, gamma-, and
delta-tocotrienol were included. Diabetic patient of any age bracket
and of either type I or type II were enrolled for current systematic
review. Besides this meta-analysis, systematic review, randomized
control trials, original articles, and guidelines published in impact
factor journals in last 05 years were also included.
While exclusion criteria were the editorials, letter to editor, case
reports, commentary, case series report and short communications.
The animal studies, ecological studies, RCTs without having placebo
or control group were also excluded.
Results
The salient results extracted from the appraisal of 05 selected articles are shown in Table IA. By following PRISMA guidelines and based upon the inclusion and exclusion criteria of study, 05(N) articles were short listed. The standardization of data was done by following critical appraisal skill program (CASP) checklist. Amongst 05 (N) selected articles, 04(n) were the randomized control trials and one was original research article. All of these 04(n) were the registered ones having details for registration bodies and numbers, It is incorporated in Table IA.
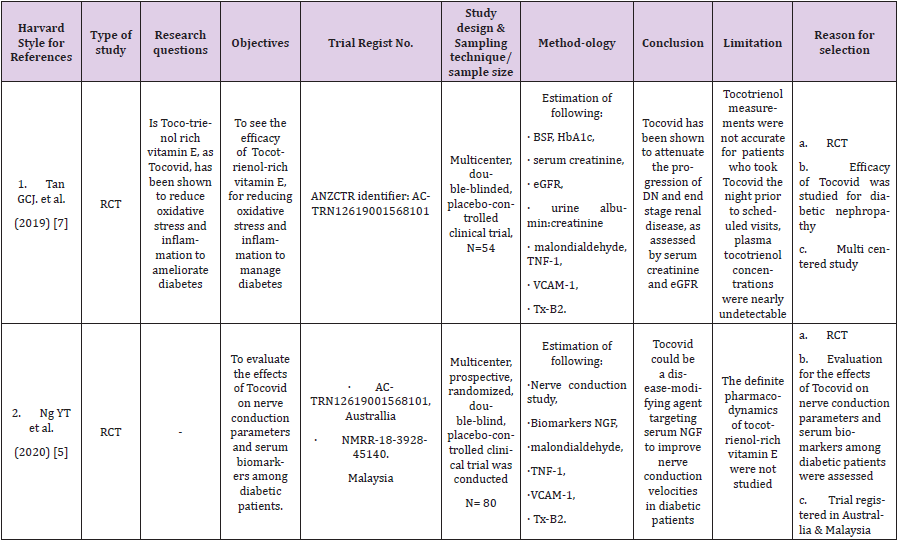
Table 1.
Despite thorough search from 08 search engines and >86
articles, no data was available showing comparative analysis for
tocotrienol and a tocopherol on diabetes patients especially insulin
resistance cases. Moreover no data was available for identifying
the efficacy of tocopherol for diabetes. Therefore, this became a big
limitation of study. Only 01(n) original article which is included as
well had shown efficacy of tocotrienol for diabetic patients with
insulin resistance. The research question was only available for
01(n) RCT. The objectives of most of these RCTs were to evaluate
the effects of high dose tocotrienol in disease outcome in diabetic
patients. Maximum follow up time was <03 months. For all RCTs, the
base line labs were done at the beginning of study. Upon completion,
they were repeated for comparison. The lab investigations included
fasting blood sugar, HbA1c, liver function tests, renal function
tests, urine albumin creatinine ratio, e GFR, malondialdehye,
thromboxane A2 (TXA2), Vascular cell adhesion molecule (VCAM),
advanced cell glycation end product (AGE), soluble receptor for
AGEs(sRAGE), Nε-Carboxy-methyllysine (Nε-CML), Cystatin C,
α-tocopherol concentration and insulin concentration by HPLC and
ELISA.
The conclusion of all 05 articles was in line with the objectives
and titles showing significant efficacy of tocotrienol for diabetes
management. The ethical issues, consent details, funding sources,
conflicts of interests, acknowledgements and authors contribution
were mentioned in every selected article.
Discussion
After a thorough search, it was assessed that tocotrienols have
antioxidant and anti-inflammatory properties. Due to which they
are strongly recommended to be a part of diabetes management
in view to reduce the serious complications of disease. The
supplementation of vitamin E had proven to be beneficial for
delaying the course of illness in diabetic patients. But the dose
variation and hence accurate dosage identification is yet to be
discovered.
Diabetes mellitus (DM) is a chronic metabolic disorder, which
might have genetic and environmental factors as predisposition.
(Study et al., 2020) It involves about 425 million people Globally.
It is expected to be increased to 629 million by the year 2045.
Therefore, the American Diabetes Association (ADA) and the
European Association for the Study of Diabetes (EASD) came up
with a consensus that management of type II diabetes mellitus
(T2DM) should focus more on life-style modification along with use
of vitamin and micro- nutrient supplementation. But this all should
be in addition to the therapeutic management. The supported
evidence is available and is proven from all 05(n) included studies
that oxidative stress plays an important role in the pathogenesis and
aggravation of DM. This is in line with the published literature which
had shown the beneficial effects of using antioxidants specially to
delay the occurrence of diabetes complications. The endothelial
dysfunction is a main pathogenesis for macro and microvascular
diseases such as retinopathy, nephropathy, lower extremity
amputations, coronary artery and cardiovascular diseases. The
scenario further worsens by the destructive properties of oxidative
stress due to free radicals of oxygen and reactive oxygen species
(ROS). This is the site of target for antioxidants like for currently
extracted evidence and available literature. Antioxidants like
tocotrienol helps their modification either enzymatically or nonenzymatically.
5 In one more study efficacy of tocopherol was
mentioned as compared to tocotrienol. This is in view that it is the
superior isoform of vitamin E. However, the further details were
deficient in that particular study to justify this [7].
The pre and post lab investigations to compare disease outcome
were done by various tests. They include fasting blood sugar,
HbA1c, liver function tests, renal function tests, urine albumin
creatinine ratio, e GFR, malondialdehye, thromboxane A2 (TXA2),
Vascular cell adhesion molecule (VCAM), advanced cell glycation
end product (AGE), soluble receptor for AGEs(sRAGE), Nε-Carboxymethyllysine
(Nε-CML), Cystatin C, α-tocopherol concentration
and insulin concentration by HPLC and ELISA. This is in favour of
many studies, which supports that diabetes complications can be
evaluated by these mentioned predictors [7].
The source for tocotrienol-rich vitamin E also came under a
debate. The one extracted from palm oil (Tocovid) was found to
improve diabetes via its superior antioxidant, antihyperglycemic,
and anti-inflammatory properties. In 04(n) studies for current
systematic review, the extract of palm oil was used. Only one study,
the source was a nut oil. This finding is supported by published data
showing efficacy of Tocovid for diabetic nephropathy in patients
with T2DM. The parameters used to assess this were HbA1c, blood
pressure, Advanced Glycation Endproduct (AGE), soluble receptor
for AGE (sRAGE), Nε-Carboxymethyllysine (Nε-CML), and Cystatin
C. 5 Another study also supported the efficacious use of palm oil
extracted Tocovid for diabetic peripheral neuropathy (DPN). This
is due to its anti-inflammatory and anti fibrolytic property, which
helps reduction of nerve growth factor (NGF). Thus, neuronal
functions will be enhanced, ultimately improving nerve conduction
velocities [8].
Amongst the predisposition of diabetes, obesity, chronic
inflammation and increased oxidative stress are key factors to
worsen the disease. They might trigger cells exposure to insulin
resistance and pancreatic β-cell dysfunction. Tocotrienol, as a
functional food component with anti-inflammatory, antioxidant,
and cell signaling-mediating effects, can be a potential agent to
supplement the management of obesity and diabetes. Tocotrienol
also improve glucose homeostasis. The activation of peroxisome
proliferator-activated receptors were the responsible one for these
effects [9,10].
The analysis of all 05(N) articles showed a dose range between
200mg to 400mg for a period of maximum 8 – 12 weeks. The
variation was there but the beneficial effects were observed in all
included studies. The same is supported by available literature that
ideal dose range should vary between 200-400mg. 11 The different
finding was observed where duration of study was 24 weeks and
430mg olive oil extract as a source of totoctrienol was used and
significant effects were observed to improve quality of life for
diabetic patients [11,12].
Conclusion
Tocotreinol because of its antioxidant, anti-inflammatory and anti fibrolytic properties helps marinating the glycemic levels in diabetic patients. Besides this the emergence of diabetic complications was delayed. A clinical improvement in patients with diabetic nephropathy and neuropathy was seen as well. It was also observed that grape seed oil supplement of tocotrienol was proven beneficial as compared to sunflower oil supplement especially by lowering inflammatory markers.
For more
Articles on : https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.