Acral Calcified Angioleiomyoma Along with Radiological Features
Introduction
ALM typically occurs in the cutaneous, subcutaneous tissue of the lower extremities in middle-aged women [1]. The author has previously described the solid subtype of ALM as a painful and vascularized subcutaneous tumor [2] and indicated that all painful cutaneous and subcutaneous tumors used as the acronym “ENGLAND” or “LEND an EGG” [3] show vascularized appearances on high-resolution color Doppler US [4]. The author also indicated that little vascularity and adjacent vessel features on color and power Doppler US and enhancing structures on one or both ends of the mass on magnetic resonance imaging may be a potential diagnostic finding in solid subtype [5]. While ALMs of the fingers, toes, hands and fee as acral type, so called acral calcified ALMs have been rarely reported. Kacerovska et al. [6] mentioned that the lesion was microscopically composed of mature smooth muscle cells and vascular pattern accompanied with focally dilated blood vessel. The prominent calcifications were observed. Recently, Suarez- Penaranda et al. [7] have reported 3 cases of acral calcified vascular leiomyoma. In this article, the current knowledges of acral calcified ALMs along with radiological features will be reviewed. In addition, the author also describes the tumors accompanied with the regions of calcification such as pilomatricomas and venous malformations in the differential diagnosis.
Characteristic Manifestations of ALM As Painful and Vascularized Tumors
ALM is a rare tumor that arises from the tunica media of small arteries and veins [1]. ALM typically occurs in the cutaneous, subcutaneous tissue of the lower extremities in middle-aged women while venous subtype tends to occur on the head and neck location in male. The painful tumors of the skin as “LEND AN EGG” including leiomyoma, eccrine spiradenoma, neuroma, dermatofibroma, angiolipoma, neurilemmoma, endometrioma, glomus tumor, and granular cell tumor have been suggested in the dermatology [3]. The acronym “LEND AN EGG” shows “ENGLAND” entity associated with endometrioma and glanular call tumor. Histological appearances show a proliferation of smooth muscle cells and vascular channels and the classification into three histological subtypes such as solid (or capillary), cavernous, and venous types have been defined [1].
Ultrasound in Dermatology
A 15 MHz is the minimum frequency recommended for performing dermatologic examination by DERMUS (Dermatologic Ultrasound), namely the international working group [8,9]. Hwang et al. [10] have reported the diagnostic value of gray scale and color Doppler ultrasonography (US) with 5-15 MHz probe in benign subcutaneous lesions. Recently, the study using the ultra-highfrequency ultrasound in the evaluation of pediatric pilomatricoma has been reported [11]. The author usually performs US studies for dermatologic fields with a high-resolution, broad-band (5MHz- 18MHz) linear transducer (Nobulus Hitachi, Ltd.Tokyo, Japan) and described several reports in the dermatologic area [2,4,5,12-24].
US and MRI Aappearances in Angioleiomyoma
The author has previously described the solid (or capillary) subtype of ALM as a painful and vascularized subcutaneous tumor, probably in close to the dermis [2] and indicated that all painful cutaneous and subcutaneous tumors including ALM used as the acronym “ENGLAND” or “LEND an EGG” [3], especially, angioleiomyoma, eccrine spiradenoma, schwannoma, and glomus tumor show vascularlized appearances on high-resolution color Doppler US [4]. The author also described the subtypes of subcutaneous angioleiomyoma on high-resolution color Doppler ultrasonography along with MRI appearances [5]. In solid subtype, little vascularity and adjacent vessel features on color and power Doppler US and enhancing structures on one or both ends of the mass on magnetic resonance imaging may be a potential diagnostic findings as previously described [5]. Regarding the magnetic resonance imaging features, some reports described that the MRI appearances of ALM have been observed as a well-circumscribed mass with an isointense or slightly high signal intensity relative to the muscle on T1-weighted images and a heterogeneous and high signal intensity on T2-weighted and short tau inversion recovery (STIR) images [25,26]. Kumar et al. [27] mentioned that diffuse homogeneous enhancement of the mass lesion with a vessel converging on the superior pole of the mass lesion was shown on postcontrast fat suppressed T1-weighted images. Kang et al. [28] described that slightly high signal intensity on T1-weighted image, a heterogeneous and high signal intensity on T2-weighted and STIR images, and heterogeneous enhancement on enhanced T1- weighted image were shown. In addition, enhancing structures on one or both ends of the mass on MRI has been reported.
Acral Calcified Angioleiomyoma
ALMs of the fingers, toes, hands and fee as acral type are rarely found. The studies of acral locations with extensive calcification including interphalangeal distal joint of the hand, sole of the foot and heel have been reported [6]. Kacerovska et al. [6] mentioned that the lesions were microscopically a neoplasia composed of mature smooth muscle cells and vascular pattern associated with focally dilated blood vessel. The prominent calcifications were observed. They also noted that the regressive changes including prominent fibrosis, calcification, and ossification are common in acral calcified ALM. Whereas ordinary ALM rarely represents these manifestations. The rare variant of ALM namely acral calcified ALM has been previously described in the literature [29-31]. The report by Gomez-Bernal et al. [32] suggested that the incidence of calcified ALM in their series is 2.5%. Some authors have suggested calcification due to a degenerative change occurring over a long period, whereas others have indicated it caused by repetitive traumas [6,29,32]. A rare case of acral calcified ALM with macroscopic calcium extrusion has also been reported [33]. They suggested that the rare histologic variant of ordinary cutaneous ALM represents a non-malignant degeneration, namely dystrophic calcification of the tumor itself [33].
Pathologically, characteristic features of ALM are a proliferation of smooth muscle bundles arising from vascular structure, thereby that vascular thrombosis, hemosiderin deposition, hyalinization, and focal calcification are not common appearances [34,35]. In addition, extensive calcification masquerading the real nature of the tumor is highly unusual [6]. Hammod et al. [36] described that the heel was the most common affected region in the lower extremity tumors, whereas the digits were the most common involved location of upper extremity tumors. The report has also suggested that digital ALM differ from acral ALM increased tendency to cause pain and preponderance for the fingers over the toes [36]. Suarez- Penaranda et al. [7] recently have reported 3 cases of acral calcified vascular leiomyoma and described two cases associated with highly uncommon appearances including trans-epidermal calcium elimination and concomitant calcaneal spur. The report by Sabater- Marco et al. also described a case of an acral angioleiomyoma with tumoral calcinosis representing a complication of the insertional Achilles tendinopathy [37]. Suarez-Penaranda et al. have also reviewed 31 acral calcified vascular leiomyoma reported in the literature and suggested that angioleiomyomas (ALMs) located in distal lower extremities tend to show widespread calcification [7]. With respect to the pain, pain is a common complaint in ordinary ALM, and it seems to be also commonly present in acral calcified ALM [7].
They concluded that calcification could be explained continuous trauma attributable to their acral location [7]. Though pathologically, characteristic manifestations in acral calcified ALM have been reported and established, the US and MRI features has not been bibliographically reported in detail. Figures 1-4 represent the features of 69-year-old female pathologically diagnosed as an acral angioleiomyoma with multiple calcified regions in her heel. Gray scale US features showed a circumscribed, relatively homogeneous hypoechoic lesion. Multiple spotty high signals which correspond to the presence of the calcification were depicted. The size of the nodule is 10 mm in depth and 16 mm in width. Rich dilated and blood flow signals in nodule were detected on color and power Doppler US. Fine flow also showed marked dilated and blood flow signals (Figure 1). On Real-Time Tissue Elastography (RTE), the nodule was depicted as relatively soft nature mass. Hemangioma, angioleiomyoma, and pilomatricoma were suggested as differential diagnosis based on comprehensively US study, especially the presence of rich blood flow signals and multiple small calcifications. On axial view, MRI appearances represent low signal intensity on T1WI (Figure 2) and high signal intensity on T2WI. The lesion of the inhomogeneous and relatively high signal intensity was shown on STIR (Figure 3). Pathologically, the lesion shows well-defined margin, fascicular proliferation of spindle cell without atypical features. The hyalinization, bleeding, and multiple calcifications were also observed (Figure 4). The nodule pathologically corresponds to the diagnosis as an acral calcified ALM.
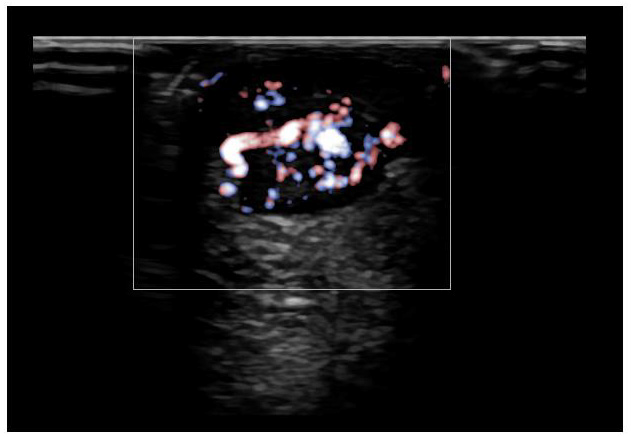
Figure 1: 69-year-old female pathologically diagnosed as an acral angioleiomyoma with multiple calcified regions in her heel. Gray-scale US features showed a circumscribed, relatively homogeneous hypoechoic lesion associated with multiple spotty high signals. The size of the nodule is 10 mm in depth and 16 mm in width. Fine flow also showed marked dilated blood flow signals.
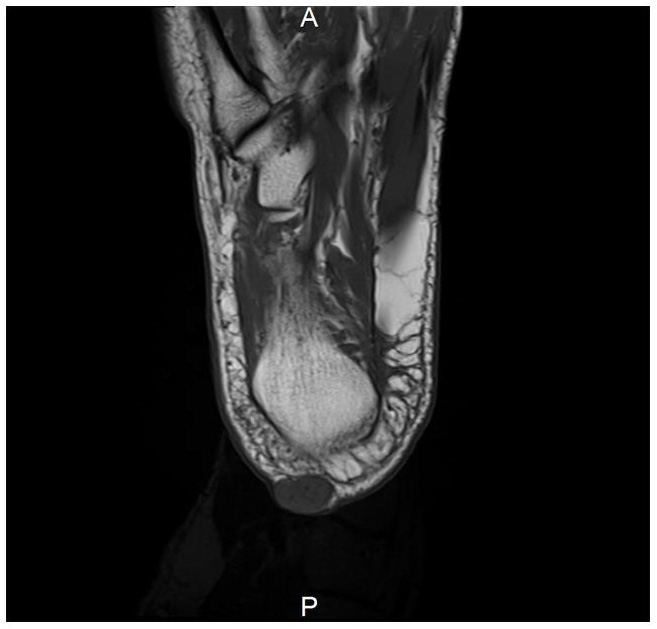
Figure 2: On axial view, MRI appearances represent low signal intensity on T1WI.
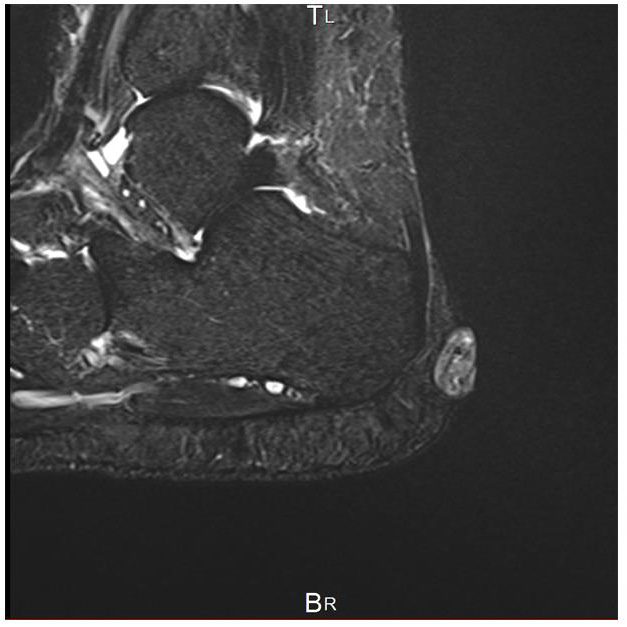
Figure 3: The lesion of the inhomogeneous and relatively high signal intensity was shown on STIR.
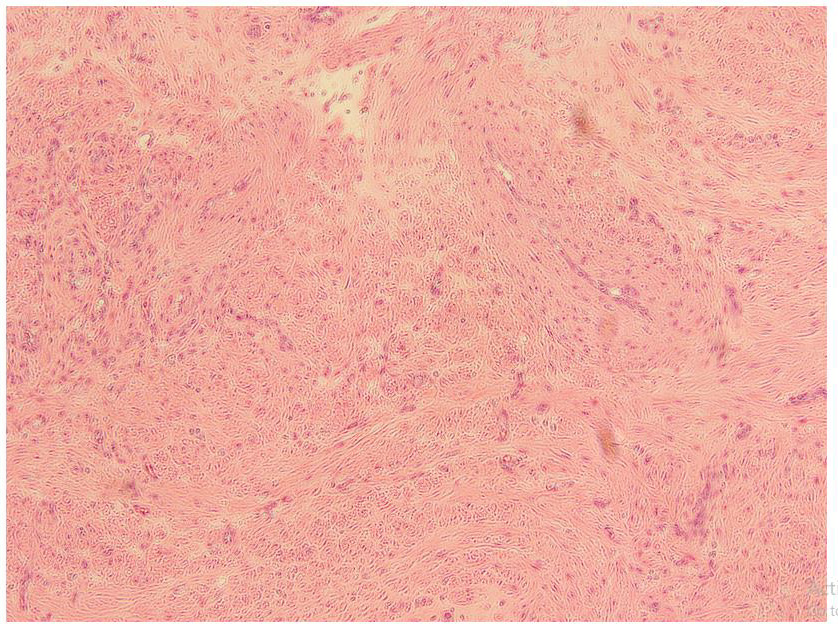
Figure 4: Pathologically, the lesion shows well-defined margin, fascicular proliferation of spindle cell without atypical features and proliferation of the blood vessels. The hyalinization, bleeding, and multiple calcifications were also observed (hematoxylin and eosin, original magnification X100).
Differential Diagnosis
Regarding the cutaneous painful and vascularized tumors in ALM, I have previously described [2,4,5]. In this article, the author mentioned the differential diagnosis focusing on the tumors accompanied with the regions of calcification such as pilomatricomas and venous malformations. Pathologically acral calcified ALMs accompanied with calcified regions have been established. Appearances of the calcified regions were depicted as strong echo with acoustic shadow on gray-scale US. Whereas the features of MRI microlithiasis represents scattered tiny signalvoid dots in calcifying aponeurotic fibromas (CAFs). The report by Kang et al. concluded that a CAF should be considered a differential diagnosis if a soft tissue mass abutting or encasing the tendon or fascia shows microlithiasis on US and MRI features [38].
Pilomatricoma
Genetically, a mutation in exon 3 of the β-catenin gene (CTNNBI) has been recognized in most human and murine pilomatricomas [39]. It has been known that pilomatricoma most frequently occurs in the head and neck location [40]. Bulman et al. performed the ultrasound imaging for 58 of the 90 lesions and indicated that seven (12.0%) lesions were densely calcified accompanied with extensive posterior acoustic shadowing. Wortsman X [41]. mentioned that hyperechoic spots that correspond to calcium deposits are shown at the center of the lesion in 68% to 80% in patients with pilomatricoma. Lin et al. [42] reported that 62.7% of the lesions were hypoechoic masses with internal calcifications.
Venous Malformation
shows variable heterogeneous echogenicity depending on the different components. Color Doppler US shows increased inner flow in vascular channel of the lesion. Hyperechoic foci with acoustic shadowing showing phleboliths may be observed [43]. Wortsman X. suggested that hyperechoic spots that correspond to phleboliths can be more commonly depicted in patient with venous malformation [41]. International Society for the Study of Vascular Anomalies (ISSVA) classification for vascular anomalies has updated in 2018. Vascular anomalies are divided into vascular tumors and vascular malformations including lymphatic, capillary, venous, arteriovenous, and mixed malformations [44]. According to Olivieri report, superficial venous malformation (VM) shows heterogeneous echotexture (98%) on gray scale US [45]. Although the finding is highly suggestive of VMs, previous report described that calcified pheboliths were seen in only 16% in pediatric and young adult patients [45,46].
In summary
Acral calcified ALMs have been rarely reported. Based on the evidence, acral calcified ALMs pathologically show the regressive changes. Similar to the ordinary ALM, it is plausible that acral calcified ALM also tends to represent painful and pathologically vascular tumors. The author mentioned the tumors accompanied with the regions of calcification such as pilomatricomas and venous malformations using high-resolution ultrasonography and MRI procedures in the differential diagnosis. In addition to the characteristic manifestation of painful and vascularized tumor on color Doppler US, acral calcified ALM should be considered as differential diagnosis if the mass shows the presence of the calcification on high-resolution ultrasonography in the acral regions.
Conclusion
a) Based on the evidence, acral calcified angioleiomyoma pathologically shows the changes including calcification, sometimes extensive calcification, hyalinization, and bleeding.
b) Acral calcified angioleiomyoma also tends to represent the painful and pathologically vascularized tumor.
c) In addition to the characteristic manifestation of painful and vascularized tumor on color Doppler ultrasonography, acral calcified angioleiomyoma should be considered as a differential diagnosis if the mass shows the presence of the calcification on high-resolution ultrasonography in the acral regions.
| For more Articles on : https://biomedres01.blogspot.com/ |




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.