A Case of Portal System Formation by Direct Joining of the Inferior Mesenteric Vein with the Superior Mesenteric Vein Observed in Anatomy Practice
Introduction
The inferior mesenteric vein (IMV) in humans flows into the portal vein (PV). In addition to the IMV, major veins constituting the portal system flowing into the PV include the superior mesenteric vein (SMV) and splenic vein (SV), and anomalies are frequently observed upon the joining of each vein. Anomalies have been also reported in gross anatomical studies [1,2,3] and on computed tomography (CT) [4-8]. Normally, the IMV ascends on the dorsal surface of the parietal peritoneum, distributes in the dorsal surface of the transverse colic attachment site, and enters the inferior margin of the pancreas, from where it flows into the SV, connecting to the PV. Regarding anomaly of this inflow region, there are 3 types: Type A directly flowing into the SV, Type B flowing into the SV/SMV junction, and Type C directly flowing into the SMV (Figure 1).
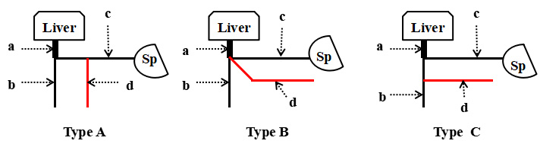
Figure 1: Inferior mesenteric vein 3 variations
• Type A) Variation of the venous drainage pattern of the inferior mesenteric vein into the splenic vein
• Type B) Variation of the venous drainage pattern of the inferior mesenteric vein into the junction between the splenic vein and the superior mesenteric vein
• Type C) Variation of the venous drainage pattern of the inferior mesenteric vein into the supeiror mesenteric vein.
a. Portal vein
b. Superior mesenteric vein,
c. Splenic vein
d. Inferior mesenteric vein
e. Sp: Spleen
In gross anatomical reports, Types A, B, and C accounted for 37, 21, and 42% of 112 autopsied bodies, respectively, in a report from Weinhaus [1], 65, 18, and 12% of 85 autopsied bodies, respectively, reported by Zilaie [2], and 73, 20, and 6% of 11 autopsied bodies reported by Kaur [3]. In CT reports, Types A, B, and C accounted for 54, 17, and 27% of 300 cases, respectively, in a report from Papavasiliou [4], 56, 18, and 26% of 54 cases, respectively, reported by Graf [5], 68.5, 7.60, and 18.50% of 102 cases, respectively, reported by Sakaguchi [6], 48.5, 10.6, and 40.9% of 66 cases, respectively, reported by Arimoto [7], and 40, 30, and 20% of 916 cases, respectively, reported by Krumm [8], demonstrating a slight difference in the frequency of each type (Table 1).

Table 1: Drainage site of IMV and frequency of occurrence. IMV= inferior mesnteric vein, SV= splenic vein, SMV= superior mesenteric vein, GA= gross anatomy, CT= computed tomography.
We report a case of direct joining of the SMV constituting the portal system in a corpse observed during anatomy practice. Embryologically, partial atrophy and disappearance of the venous system occur from the bilateral vitelline veins and their anastomotic branches as the intestine rotates at approximately 6 weeks of embryogenic age [9-12]. At this time point, a certain abnormality may have occurred when the distribution of bilateral vitelline veins started to become that observed in adults around the intestine through their development and regression, forming an anomaly in the IMV inflow region.
Case Report, Observed Body and Methods
The anomaly of the IMV noted in an 89-year-old female (autopsy number 1989: senility) donated to Kanagawa Dental University for anatomy practice in the fiscal year of 2019 was excised using gross anatomical techniques, and the SMV, IMV, SV, and spleen were excised while connected to the PV (Figure 2). This report was prepared based on the ethical codes of the Japanese Association of Anatomists after approval (approval number: 557) by the Kanagawa Dental University Research Ethics Committee. There was no COI-related organization or institution.
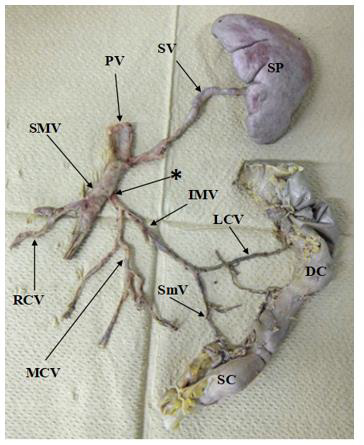
Figure 2: Anatomic variants of the inferior mesentric vein (IMV): reaely drainage of the IMV into the superior mesentric vein (SMV) can be found. SP= Spleen, DC= Descending colon, SC= Sigmoid colon, PV= Portal vein, SV= Splenic vein, SMV= Superior mesenteric vein, IMV= Inferior mesenteric vein, MCV= Middle colic vein, RCV= Right colonic vein, LCV= Left colonic vein, SmV= Sigmoidl vein, *= Location of the IMV drained into SMV.
Results
The SV from the splenic hilum ran on the top surface of the pancreas on the posterior surface of the gastric corpus and flowed into the PV. The right and middle colic veins joined the SMV and flowed into the portal vein. In addition, the IMV joined by the jejunoileal vein joined at a site approximately 2 cm distal to the SPV from the region of the SMV and SV flowing into the PV (Figure 2).
Discussion
The portal vein is a functional blood vessel related to functions, such as detoxification and metabolism in the liver and bile production. The main veins constituting the portal system are the SMV, which transports nutrients absorbed in the jejunum and ileum, and water absorbed in a part of the ascending and transverse colon to the portal vein, the IMV, which transports water absorbed in the rest of the transverse, descending, and sigmoid colon and upper rectum, and the SV, which transports a component of red blood cells destroyed in the spleen, indirect bilirubin. Nutrients ingested by humans start from the oral cavity, are absorbed in the small and large intestine, and stored in the liver through the portal system. The portal system plays an important clinical role in absorption, metabolism, and storage of nutrients [13,14]. In addition, an increase in venous blood flow of the portal system was suggested to alter intrahepatic blood flow components of the portal vein, reducing the hepatic functional reserve. An anomaly was noted in this gross anatomical observation, in which the IMV joined the SMV and flowed into the portal vein. Anomalies of blood vessels constituting the portal system slightly differ among reports [1-8] but as shown in Table 1, the mean frequency of Type C in which the IMV directly joins the SMV was 24.1%.
Many veins constituting the digestive system gather in the portal vein and congenital abnormality in the distribution of the portal vein is considered markedly rare, even though the embryological timing is the same as that of the bile duct and celiac artery system. During development of the portal vein, 2 vitelline veins that develop from the yolk sac at 4 weeks of embryogenic age distribute to be positioned on the bilateral sides of the archenteron, which becomes the future duodenum, and then join the main vein and umbilical vein, and flow into the venous sinus. At 5 weeks of embryogenic age, 3 anastomotic branches of the bilateral vitelline veins on the cranial side, middle anastomotic branches, and anastomotic branches on the caudal side are formed on the ventral or dorsal side of the archenteron. At 6 weeks of embryogenic age, the venous system partially starts to atrophy, and disappears from the bilateral vitelline veins and their anastomotic branches as the intestine rotates [9-12]. At this time point, a certain abnormality may have occurred when the distribution of the bilateral vitelline veins around the intestine started to become that observed in adults through development and regression and formed an anomaly in the IMV inflow region. It has recently become possible to acquire detailed information before surgery due to the development of imaging diagnostic methods, including angiography, in all fields, thus increasing the frequency of surgical approach to the portal system in the digestive field. By identifying abnormalities in the distribution of the portal system before surgery, decisions regarding the surgical approach to the portal system can be easily made and its limitations are known.
For digestive surgery, CT is essential for treatment, and abnormality of the portal system distribution can be accurately diagnosed by ultrasonography and angiography in addition to CT, being a promising auxiliary diagnosis. Moreover, there are many case reports of abnormality of the portal system distribution based on imaging diagnosis [4-8]. It is necessary to identify the venous system from venules originating in the jejunoileum and colon that join the main veins of the portal system, i.e., the SMV, IMV, and SV, to investigate not only approaches in digestive surgery, but also the states of liver function and nutrition in patients in all fields. For anomalies of the portal system, confirmation on imaging, and gross and clinical anatomical information are desired.



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.