Occult Lung Cancer with Acrometastatic Presentation: A Case Report
Introduction
Digit tumors of the hand are uncommon clinical conditions. Differential diagnosis of these lesions can cross over more common conditions, like infection or swelling and always requires histological examination. [1-15] The first clinical examination often occurs in emergency room (ER), since pain, swelling and functional impairment are common symptoms [2,11]. In this report we describe a case of a rare acrometastasis that turned out to be of pulmonary origin. Metastasis at hands and fingers is a rare entity, but even rarer is their presentation as the first sign of a cancer [1,3]. Dominant hand is slightly predilected and the distal phalanx of the thumb is the most frequently involved location [1]. The prognosis is unfavorable, the average survival from the time of diagnosis is about 7 ± 7 months, although extremely rare cases of longer survival are described [4,8,14].
Clinical Case
A 61-year-old man came to our emergency room because of worsening pain and swelling in his left thumb started one week before. The patient did not present fever and symptoms did not regress after empirical treatment with a broad-spectrum antibiotic prescribed by his general practitioner. He reported to be a smoker (20 cigarettes a day) and denied recent trauma or other comorbidities. Under local anesthesia, the lesion was incised, but no serous or purulent secretion came off. However, the dermis layer appeared particularly thick, therefore a lozenge of tissue was taken for histological examination. The X-ray of the hand (Figure 1a) showed an area with erosive features and cortical osteolysis of the distal phalanx of the first finger. Blood chemistry tests showed an increase in ESR (59 mm/h) and CRP (31.4 mg /L) Chest X-ray (Figure 1b) reported. “Good lung expansion with isolated dystelectatic streak in the right upper peri-hilar area. No active pleural-parenchymal lesions. Hila of vascular type. Heart’s dimensions within the normal limits. Aorta with isolated, thin parietal calcification at the arch. Moderate segmental swelling of the dorsal soft tissues at the upper 3rd – middle 3rd passage of the thoracic cage.”
21 days after accessing the emergency room, the patient found a painless wooden swelling in the left periscapular region on self-examination. 25 days after accessing the emergency room, the histological examination report described a suspicion between cutaneous primary malignant primitive adnexal neoplasm (adenocarcinoma not further specified) and a metastasis from adenocarcinoma of clinically unknown primitivity. The immunohistochemical survey was positive for CKAE1-3, CK7, EMA, CEA, Calretinin. Negative for TTF-1, Pax-8, S100, Napsin-A, p63, p40, D240, CDX2, PSA, Desmina, SMA. The patient was therefore hospitalized. A total body CT exam was performed, that found out a neoplastic disease with multiple locations suspected for metastases at the cervical nodes (Figure 2a) at the dorsal spine (Figure 2b) and at the liver (Figure 2c). The dorsal lesion was removed and sent to histological examination whose report was comparable to the first histological examination performed on the digit lesion, describing a lesion whose suspect was between skin adnexal malignant neoplasm and a localization of a poorly differentiated tumor not further specified. However, the immunohistochemical negativity for TTF-1 did not exclude a possible pulmonary primitivity, which appeared more likely in the light of the instrumental findings.
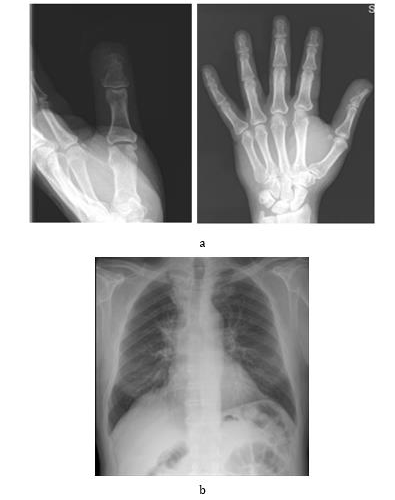
Figure 1.
Moreover, the patient underwent a gastroscopy with biopsies of the gastric muscle to exclude a gastrointestinal origin. The examination was negative for neoplastic pathologies. (Figure 2d). During the total body PET examination with fluorideoxyglucose, intense accumulation of the tracer was detected at the sites identified bythe CT, in the Barety’s space and in the pulmonary hilar area (Figure 2e). Therefore, a neoplastic disease with probable right lung primitiveness was identified.54 days after accessing the emergency room, the thumb appeared swollen with uncontrolled pain and skin ulceration (Figure 2f). Therefore, the patient was treated with a surgical digital amputation through the proximal phalanx in order to manage local complications; the histological examination was comparable to the previous ones. Follow-up PETCT examination was performed 2 months after surgery. Aggravation of the neoplastic disease was reported, with appearance of new skeletal and splanchnic localizations. Three months after surgery occurred hemoptysis and frank progression of the pulmonary neoplastic disease (Figure 2g). The patient died at 7 months from the first access to the emergency room.
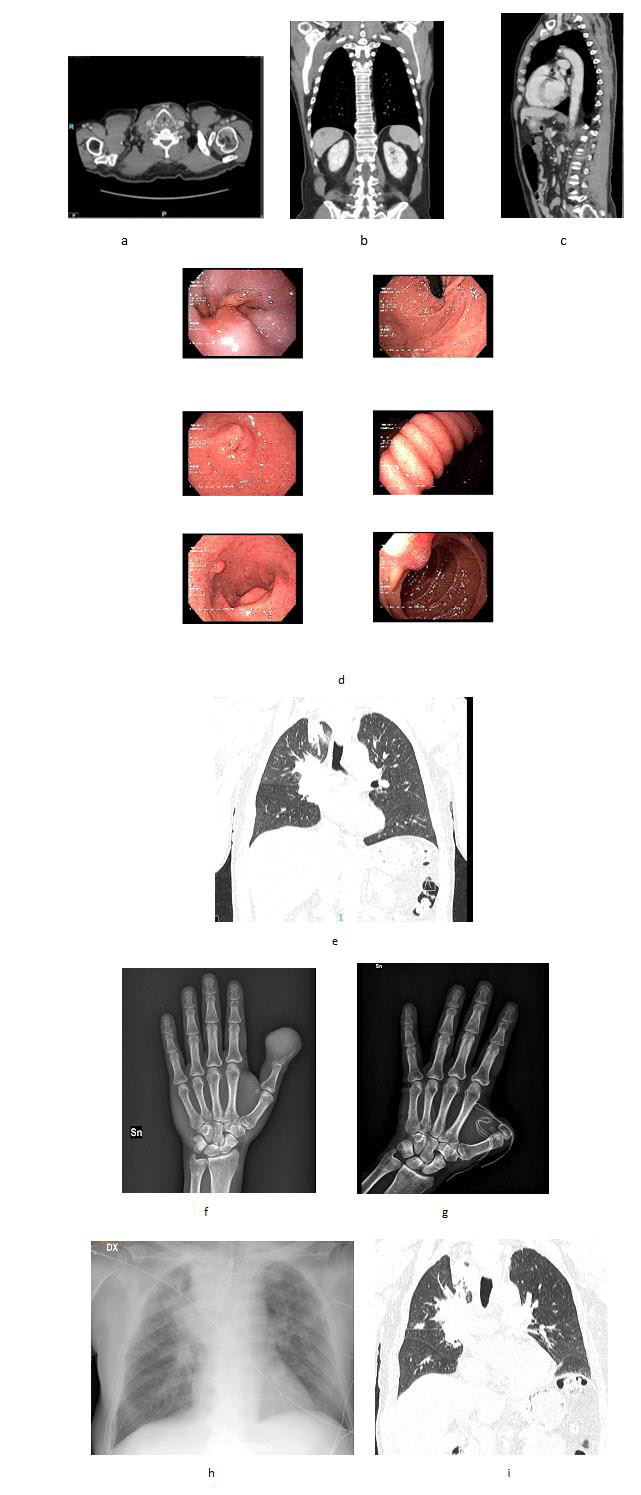
Figure 2.
Discussion
Acrometastases are rare with an incidence of 0.1% among all metastases, men are more likely to be affected than woman and the primary sites involved are lung, kidney, breast and gastrointestinal tract [1,5,12]. Acrometastases can become symptomatic before the primary tumor is identified in a percentage between 10% and 30% [1,6,9,15]. They are generally painful, can appear as an infected swelling, can ulcerate and bleed and often affect the thumb (Figure 2h). Generally, those of pulmonary origin are aggressive. Moreover, joint space is commonly preserved [7]. In our case, biopsy was essential to differentiate it from osteomyelitis or other infectious disease, but it was not diriment about the primitivity of the lesion (Figure 2i). In this context, the radiological studies were crucial to orient towards a pulmonary primitivity. The choice of a surgical treatment was therefore purely palliative. It is interesting that the suspect of an oncological condition occurred since the first visit at emergency room, despite the higher incidence of other conditions and their similarities. Probably incising the lesion turned out to be a good decision, since the absence of secretion, associated to the clinical history of the patient, oriented toward a not infectious condition [16].
Conclusion
The prognosis of an occult lung cancer with metastatic presentation in the fingers is poor. Chemotherapy and local radiotherapy can relieve the pain and regress the mass, but finger amputation may be necessary for very aggressive neoplastic diseases. Although there are not studies measuring directly the improvement of the quality of life after surgery, it is agreed that this procedure is the best way to control the pain [6,10,13]. It is important that the orthopedist and the emergency doctor has knowledge of these rare disease, in order to start a differential diagnosis and perform the right procedures.



No comments:
Post a Comment
Note: Only a member of this blog may post a comment.