Electrotherapy for the Treatment of Diabetic Distal Polyneuropathy
Introduction
Background
In many cases pharmacotherapy turned out to be ineffective in treatment of many patients with diabetic distal polyneuropathy. Clinicians in recent years have therefore begun to widely use nonpharmacotherapy to enhance the effectiveness of drug treatment of DN [1,2]. The advantages of non-pharmacotherapy methods are minimal side effects, as well as the absence of contraindications [1]. It is important to note that acupuncture and transcutaneous electroneuro stimulation were recommended by Toronto Diabetic Neuropathy Expert Group for treatment of diabetic distal polyneuropathy [1]. In many studies, the effectiveness of TENS in treatment of psychogenic, nociceptive and neuropathic pain syndromes has been proven. [3]. However, the effectiveness of TENS in the treatment of sensory and motor deficits in distal polyneuropathy was studied insufficiently [1,4,5].
Objective
To study the dynamics of sensory and motor deficiency in diabetic distal polyneuropathy syndrome by using Transcutaneous Electrical Neurostimulation (TENS) of peroneal and tibial nerves.
Materials & Methods
Our study included 60 patients with diabetic distal polyneuropathy of the lower extremities. Patients are between 35 and 65 years of age. The average age of the patients was 47 years (Figure 1). 20 patients underwent only standard pharmacotherapy. In addition to pharmacotherapy another 20 patients were managed with high frequency and Low Amplitude (HL) TENS and the rest 20 patients were treated with low frequency and High Amplitude (LH) TENS of peroneal and tibial nerves.
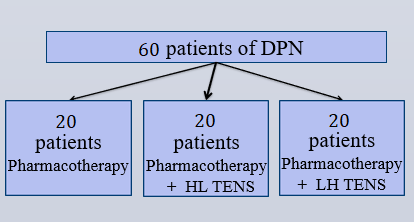
Figure 1: Distribution of patients into groups depending on the method of treatment.
Methods of Treatment
a. Pharmacotherapy: Pharmacotherapy was administered for 2 months with the use of vitamin B, Duloxitine and alpha lipoic acid (Figure 2).
b. TENS: TENS was carried out in the second month of pharmacotherapy. We used 2 variants of TENS: high frequency TENS (HL) and low frequency TENS. Characteristics of current are shown in (Figure 3).
• LH TENS: Frequency = 1 Hz. Amplitude (no painful muscular response). Duration = 200 μs.
• HL TENS: Frequency = 100 Hz. Amplitude (clear sensory response). Duration = 100 μs
Technique of TENS is shown in (Figure 4).
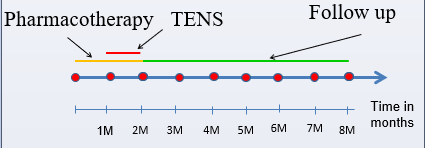
Figure 2: Observation of the treatment and outcomes of patients.

Figure 3: Characteristics of current.
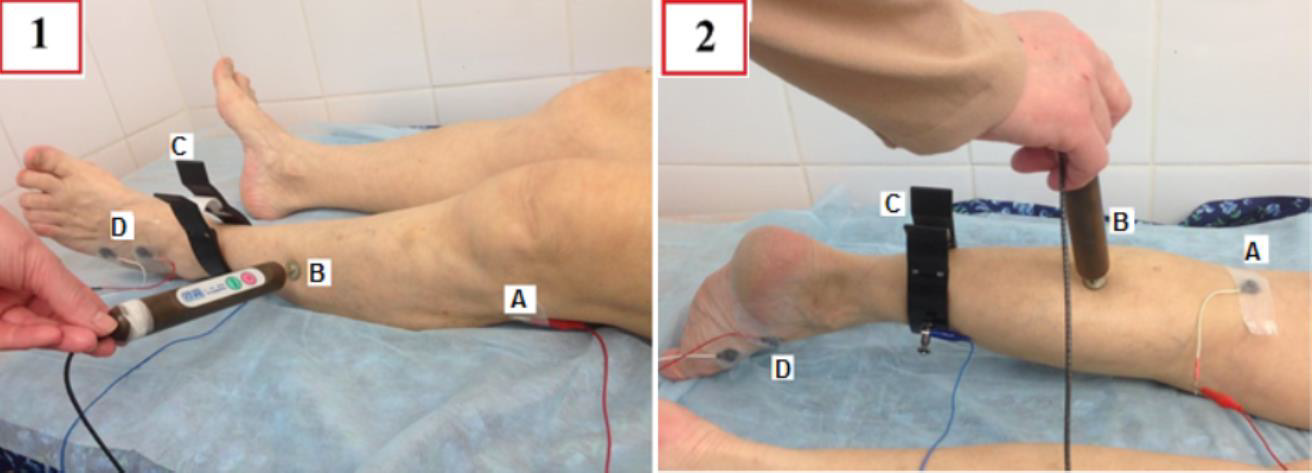
Figure 4: Technique of labile low-frequency TENS of peroneal nerve (1) and tibial nerve (2). Cathode (A) is fixed in the proximal nerve. The stimulating anode (B) is labile and has the form of a pen. Each 10 cm the anode was moved from the proximal nerve in the distal direction. The ground electrode (B) is on the lower third of the leg and the active and reference recording electrodes (D) are fixed in foot area as in EMG examination of the peroneal and tibial nerves. The course consisted of 15 procedures every other day.
Methods of Examination
To assess the degree of peripheral nerve damage against the background of distal polyneuropathy of the lower extremities and their degree of regression after the treatment and in the follow-up, we used the following diagnostic methods:
• Negative sensory symptoms: Vibration, temperature, tactile and pain hypoesthesia were determined by 5-point scales.
• Positive sensory symptoms: Subjective sensory disorders such as tingling, numbness, burning pain and shooting feeling were described by the patients themselves using 10-point scales.
• Ankle dorsiflexion strength was investigated using a 5-point scale.
• The severity of neuropathic pain syndrome was determined on a 10-point visual analogue scale (VAS).
• By electromyography conduction velocity and amplitude of M-response of peroneal and tibial nerves were examined.
Results
Pain Syndrome
significantly decreased on the background of the TENS in comparison with pharmacotherapy by 43% (Figure 5). Analgesic effect of HL TENS proved to be more effective than LH TENS by 34, 7%.In the second and sixth months of the follow-up period there were no significant differences between the various modalities of TENS (Figure 4).
Negative Sensory Symptoms
Significantly decreased as a result of the additional application of TENS by 25, 9%. Improvement of sensory disorders was noted in patients who passed LH TENS more than HL TENS by 78% (p<0,05).In the second month of the remote period after LH TENS negative sensory continued to decline significantly by 19%(Figure 5). Positive sensory symptoms significantly decreased with the use of TENS 39% more than using of pharmacotherapy alone. Positive sensory symptoms regressed after application of HL TENS in comparison with LH TENS by 24% (p<0.05).In the follow-up period positive sensory symptoms in both groups showed no significant differences (Figure 6). Recovery of motor weakness was not observed after the use of pharmacotherapy alone and was detected only after LH TENS and was on average 17% in ankle dorsiflexion and 22% in ankle dorsi extension (Figure 7) Electromyography values of M-response and velocity of peroneal and tibial nerves were not significantly changed, however, in some cases there was an improvement in the M-response rate in electromyography after LH TENS (Figure 8).
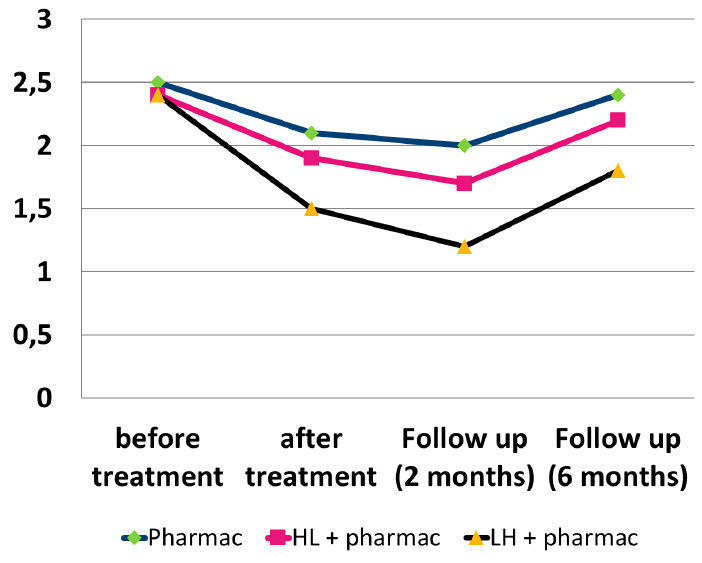
Figure 5: Dynamics of negative sensory symptoms in different periods of observation.

Figure 6: Dynamics of positive sensory symptoms in different periods of observation.
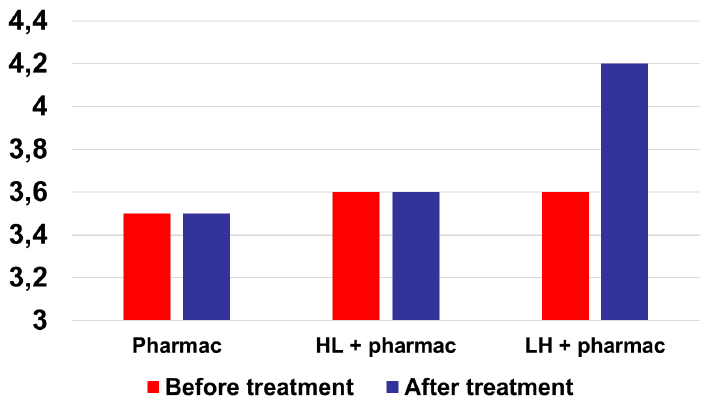
Figure 7: Dynamics of ankle dorsiflexion strength.
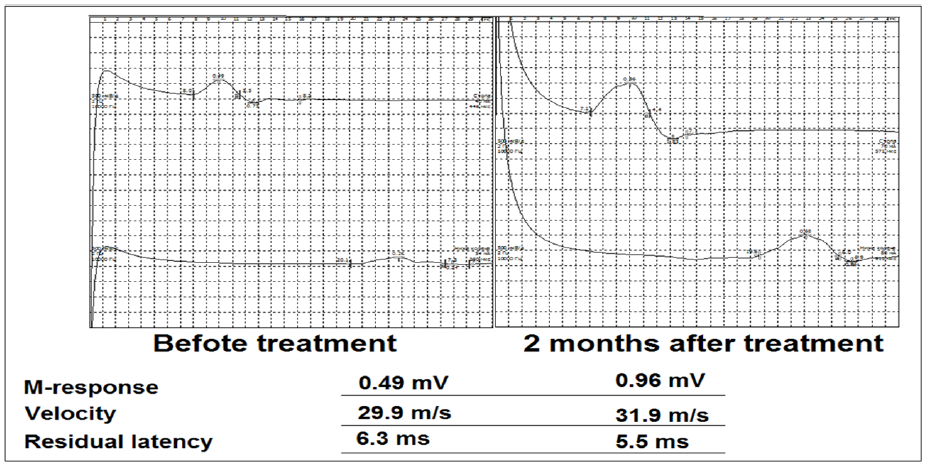
Figure 8: Electromyography dynamics of M-response and velocity of left peroneal nerve after using LH TENS in treatment of patient with diabetic distal polyneuropathy (woman, 55 years old and MD 12 years).
Conclusion
TENS increases the effectiveness of pharmacotherapy in the treatment of diabetic peripheral neuropathy in reducing the negative and positive sensory symptoms, motor deficit and neuropathic pain syndrome. TENS has a prolonged effect that lasts for 6 months of the follow-up period. The maximum therapeutic effect is observed in the second month of the follow-up period. High frequency-low amplitude TENS is recommended for treatment of neuropathic pain and positive sensory symptoms. Low frequencyhigh amplitude TENS is the method of choice in treatment of negative sensory symptoms and motor deficit. Recovery of electromyographic abnormalities was not observed in all patients. However, in many patients, there was a noticeable amplitude increasing of M-response.




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.