Practice of Self-Medication with Antibiotics Among the Adult Inhabitants in Dhaka City
Introduction
The World Health Organization has emphasized that selfmedication must be correctly taught and controlled as the selfmedication is a great threat for the health globally WHO, [1]. Antibiotic self-medication is highly prevalent in the developing countries due to easy availability. Resistance to commonly used antimicrobial drugs is remarkably high in countries where antibiotics are not restricted Sallam, et al. [2]. There are some other reasons like wider availability of medicine, greater choice of treatments, in preventing or reliving miner symptoms or condition, ailment was minor and financial constraint Jain, et al. [3]. Antibioticresistant infections also contribute to the financial burden on health care systems Gelband, et al. [4]. A study conducted in Bangladesh in 2014 found that 26.69% in Rajshahi city experienced self-medication with highest percentage of self-medicated medicines were metronidazole (50.43%), azithromycin (20.75%), ciprofloxacin (11.53%), amoxicillin (10.37%) and tetracycline (7.49%) respectively. The key reasons for the self-medication of antibiotics was the pre-experience (45.82%), Biswas, et al. [5]. A cross sectional study conducted in 2017 in Dhaka city found that undergraduate medical students were found to practice more selfmedication (78.1%) than the non-medical students (55.1%) Nasir, et al. [6].
Reason and Factors Influencing Self-Medication with Antibiotics
Parents medicate to their children to save money or to avoid a trip to doctor’s office Bennadi [7]. A number of reasons for selfmedication such as saving money and availability of drugs in drug shops are responsible for growing trend of self-medication Oluyemi [8]. Many studies showed that limited purchasing capability is a major determinant for self-medication with antibiotics in India, Nigeria, Philippines, Latino adults in the United States of America, and the non-Arab population in the United Arab Emirates. Pharmacy staff behavior can be a factor that puts patients at risk for self-medication with antibiotics Oluyemi, et al. [8,9]. Inappropriate Antibiotic and Nonprescription use of antibiotics can range from 19 percent to well over 90 percent outside the United States and Europe, Vietnam, in Saudi Arabia and Syria, pharmacies dispensed antibiotics without a prescription Van Boeckel, et al, [10].
OTC Drugs
Over the Counter (OTC) drugs are non-prescription drugs that are not normally covered by a Medicare Prescription Drug Plan. OTC medications are legal, non‐prescription substances taken for the relief of discomforting symptoms. Although OTC drugs are believed to be safe and effective, indeed they are not. They mask the underlying disease and may cause several adverse effects Parikh, et al. [11]. A prescription is an order that is written by the physician to tell the pharmacist what medication your patient wants to take Inlander, et al. [11,12]. Drugs that destroy microbes, prevent their multiplication or growth, or prevent their pathogenic action – Differ in physical, chemical, pharmacological properties, differ in antibacterial spectrum of activity, differ in their mechanism of action.
Worldwide Antibiotic Resistance Rates and Trends
In the United States, more than 2 million infections and 23,000 deaths are due to antibiotic resistance each year and in Europe, an estimated 25,000 deaths CDC, [13]. Antibiotic-resistant infections also contribute to the financial burden on health care systems Gelband Quet, et al. [4,14]. A vast majority (93%) of the patients were totally unaware of the possibility of side-effects Teck, et al. [15-17].
Parental Knowledge About Antibiotic Use/Discontinuation in Bangladesh
High percentage of parents thought that antibiotics could cure infections caused by viruses and also cold, fever and sore throat. Resistance to commonly used antimicrobial drugs are remarkably high in countries where antibiotics are not restricted Sallam, et al. [2]. In Bangladesh, increasing rates of antimicrobial resistance andthe prevalence of self-medication is thought to be high, as a result, minor illnesses are treated with antimicrobials which have potentially harm the individual Gutema, et al. [18- 21,3]. Many older adults independently manage their prescription and nonprescription (OTC) medications Keshari, et al. [22,23]. A majority of the prescribers diagnose infection by clinical assessment and suspect a microbial etiology Faiz, et al. [24].
Methods and Materials
The study is a Cross-sectional descriptive study andit was helpful to describe the current conditions and situations based on the impressions and views of the respondents of the study (Thomas et al., 2005). The study location was Azimpur, lalbagh, Kamrangirchar belongs to Zone-5 of Dhaka South City Corporation. These areas are highly populated, and it was feasible to find people or respondents from every economic status like lower, middle and higher socioeconomic. The total study duration was 10 months from May 2019 to February 2020.
Study Population
The target population was adult age group (18 or more than 18 years old). Both male and female were selected from any religion and socioeconomic status. Pre-tested, semi structured interview questionnaires. This balance was useful for a comprehensive analysis. Data was entered in Microsoft Excel and analysis was done by using descriptive statistics in Microsoft Excel 2010 and SPSS version 20.
Ethical Consideration
Permission was taken from Institutional Review Board (IRB) of American International University-Bangladesh (AIUB), the committee on activities involving human subjects.
Results
Distribution of the Respondents’ Socio-Demographic Variables
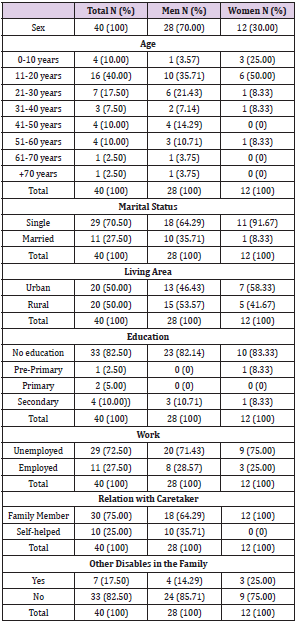
Among the total (140) participants, 37.9% participants were between the 18 and 28 years old, 33.6% between the 29 and 39 years old, 20.7% between the 40 and 50 years old, 5.7% between the 51 and 61 years old and 2.1% were 62 years and above. Among the respondents, 56.4% participants were male and 43.6% were female and among them 64.3% were married and 35.7% were unmarried. It reveals that the participants’ education level was as illiterate 6.4%, primary 10.7%, secondary 14.3%, SSC 13.6%, HSC 15.0%, graduation 20.0%, masters and other higher degrees also 20%. Graduation, masters and other higher degree holder participants were more in numbers than others.
Knowledge about Antibiotic Resistance among Medicated and Non-Medicated Group
The result demonstrates that 37 participants out of 79 (46.8%) consulted doctor and other 42 participants out of 79 (54.2%) didn’t consult reg. doctor. Among the 42 participants who didn’t consult MBBS/reg. doctor 14 participants (17.7%) visited local pharmacy and took suggestion/medicines, 10 participants (12.7%) consulted quack/village doctor/medical assistant, 9 participants (11.4%) medicated from home stored medicine/family/friends, 3 participants (3.8%) consulted doctor of alternative medicine (Homeopathy/Uniani/Ayuryeda/Others) and 6 participants (7.6) did other health seeking behavior (Figures 1 & 2).
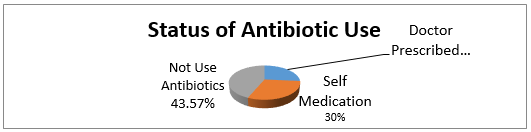
Figure 1: Status of antibiotic use in last 12 months.
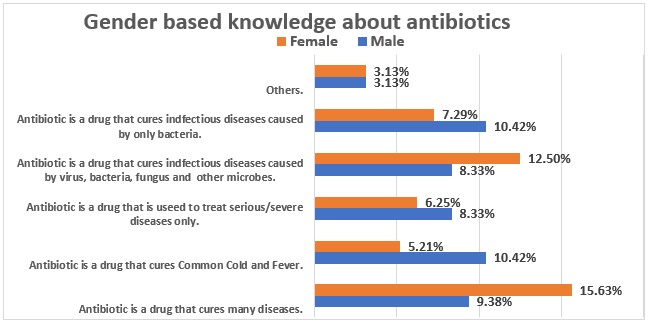
Figure 2: Gender based knowledge about antibiotics.
Antibiotics Medication and Gender
Status of antibiotic use among the antibiotic users: The rate of self-medication with antibiotics (53.16%) is higher than the use of antibiotics (Figure 3) prescribed by doctors (46.84%). Selfmedication number was higher in male (31.65%) than the female (21.52%) and alternatively the number of antibiotics prescribed by doctor was higher in female (29.11%) than the male (17.72%).
Antibiotic Medication and Education Level
Education plays an important role to grow up the level of health awareness. In this study, most of the persons whom education levels were “Primary” (11.39%) used antibiotics as self-medication in higher rate and most of the persons whom education level was “Master” (16.46%) used antibiotics as prescribed by reg. doctors in higher rate. Practice of antibiotic prescribed by doctors is gradually higher in higher education group and gradually lower in lower education group. Alternatively practice of self-medication with antibiotics is higher in lower education level and lower in higher education level (Figure 4). Practice of self-medication is higher in male persons (59.52%) and comparatively lower in female parsons (40.48%). Practice of self-medication is higher in married people (59.52%) and comparatively lower in unmarried people (40.48%). (Figure 4). Practice of self-medication is higher in lower education level (illiterate 4.76%, primary 21.43%, secondary 19.05%, SSC 16.67%, HSC 14.29%, graduation/honors 16.67% and masters and other higher degrees 7.14%).
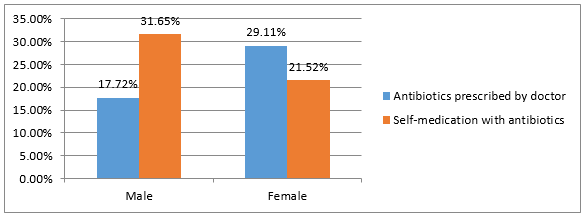
Figure 3: Antibiotics Medication and Gender.
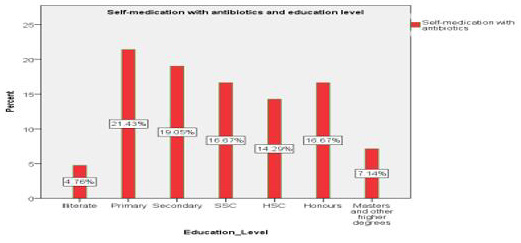
Figure 4: Self-medication with antibiotics and education level.
Antibiotic Medication and Income Level
Income is a vital factor to improve the health seeking behavior. In this study, most of the persons whom income level were BDT>40000 to 60000(15.19%) and BDT >80000(12.66%) used antibiotics as prescribed by doctor. But most of the persons whom income level were BDT<=20000(24.05%) used antibiotics as selfmedication. Practice of self-medication with antibiotics is higher in lower income level and practice of antibiotic prescribed by doctor is higher in higher income level (Figures 5 & 6).
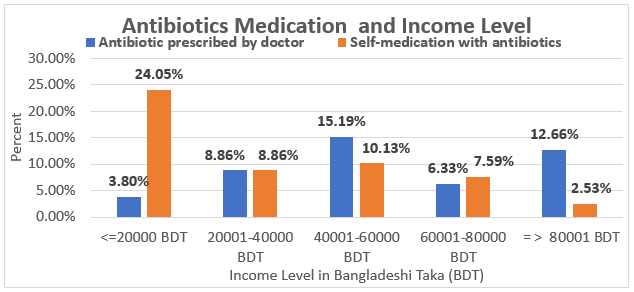
Figure 5: Antibiotic medication and Income Level.
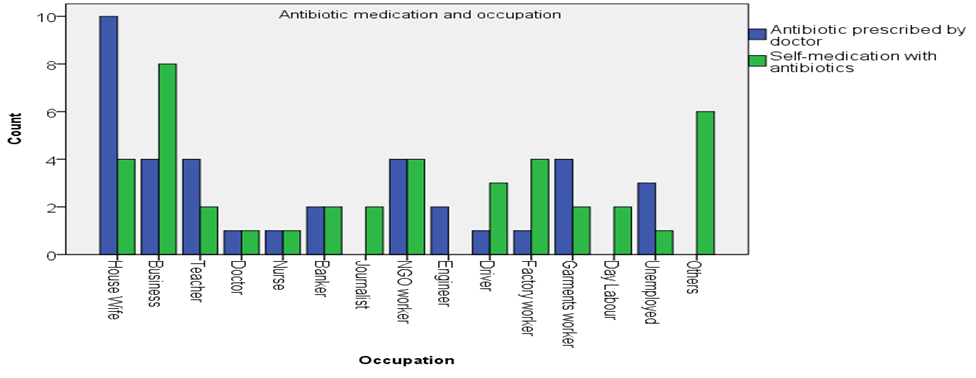
Figure 6: Medication Type and occupation among antibiotic users.
Gender and Source of Self-Medication with Antibiotics
The most common source of antibiotic for self-medication was “bought from private pharmacy without prescription” for male (38.10%) and for female (14.29%). ‘Previously stored antibiotics’ for male (11.90%) and for female (14.29%). ‘From family and friends’ for male (7.14%) and for female (9.52%) and other sources were for male (2.38%) and for female (2.38%) (Figure 7). The highest rate of used antibiotics for self-medication is Metronidazole (21.4%), secondly Ciprofloxacin (19.0%), Thirdly Azithromycin (16.7%). Cloxacillin (9.5%), Amoxicillin (7.1%), Cefixime (7.1%), Cefuroxime (2.4%), other antibiotics (2.4%) and under not sure (14.3%).
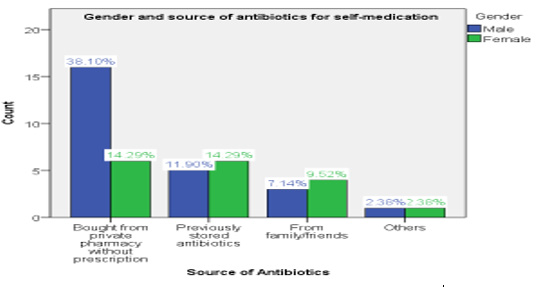
Figure 7: Gender and source of self-medication with antibiotics.
Use of Antibiotics (Self-Medication) and Diseases
Metronidazole was most commonly used for Dysentery (21.43%), Secondly Ciprofloxacin was used for Fever (11.90%) and Common cold (7.14%). Thirdly Azithromycin was used for Fever (4.76%), for Sore throat (4.76%), for Sinusitis (2.38%), for Injury (2.38%). Amoxicillin used for Common cold (4.76%) and for Cough (2.38%). Cloxacillin was used for Injury (4.76%). Cefixime was used for Sore throat (2.38%), for Cough (2.38%) and for Dental infection (2.38%). Cefuroxime was used for Sore throat (2.38%), other antibiotics were used for Dermatological condition (2.38%) and under not sure 7.14% for Fever and 4.76% for Dental Infection. Most of the people (whom taken antibiotic as self-medication) were taken antibiotic due to Dysentery fever (Figure 8).
Discontinuing Antibiotics after Starting with Self- Medication
Majority of the participants didn’t stop taking antibiotics (incomplete course of treatment) (59.52%), and some participants stopped taking antibiotics without completing the course of antibiotic (33.33%) and 7.14% participants were not sure (Figure 9).
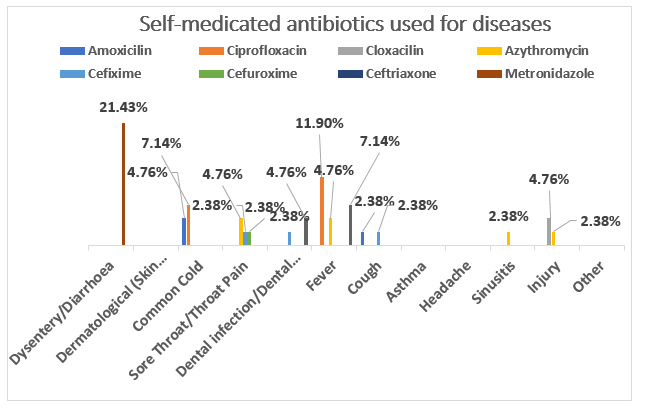
Figure 8: Use of antibiotics (self-medication) and diseases.
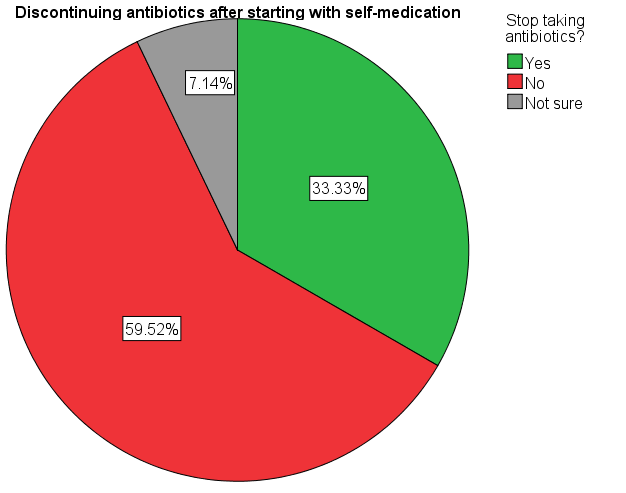
Figure 9: Continuity antibiotics after starting with self-medication.
Cure Diseases after Self-Medicating with Antibiotics
30.95% participants reported that they were not cured after taking antibiotics (self-medication) although majority of the participants 66.67% reported that they cured from diseases after taking antibiotics (self-medication), 2.38% participants were not sure (Figure 10). The association between the gender and antibiotic use and that is statistically significant (P-value = .024). There is relationship among self-medication with antibiotics group, antibiotics prescribed by doctor and no use of antibiotics group. The association between the income level and antibiotic use and that is statistically significant (P-value = .017). There is relationship among self-medication with antibiotics, antibiotics prescribed by doctor and no use of antibiotics group with income level. Practice of antibiotics varies on the income level. Income has an effect on use of antibiotic practice.The association between the education level and antibiotic use and that is statistically significant (P-value = .002). There is relationship among self-medication with antibiotics, antibiotics prescribed by doctor and no use of antibiotics group with education level. There is relationship of self-medication with antibiotics, antibiotics prescribed by doctor with education level.
The Chi square test showing that there is no association between education and self-medication with antibiotics and no use of antibiotics (P-value= .357). Statistically there is no significant. There was strong association between the education and antibiotic user prescribed by doctor and that is statistically significant (P-value = .012). There is relationship of antibiotics prescribed by doctor with education level. There was strong association between the income level and antibiotic user prescribed by doctor and that is statistically highly significant (P-value = .000). There is a strong relationship of antibiotics prescribed by doctor with income level. Practice of antibiotics prescribed by doctor varies on the income level. Higher income leads to the visit of registered doctor and proper practice of antibiotic use (prescribed by doctor).
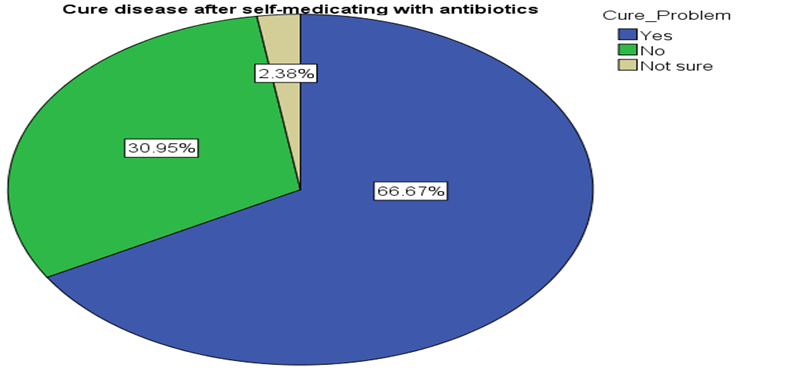
Figure 10: Rate of cure after self-medicating with antibiotics.
Discussion
A study conducted in Rajshahi city of Bangladesh in 2014 found that 347 (26.69%) out of 1300 participants in Rajshahi city experienced self-medication with antibiotics Biswas, et al. [5]. The percentage of self-medication has been increased more than previous years which is very alarming. The selection of antibiotics in a study conducted in Dhaka city found that the reasons behind the self-medication was ‘minor illness’ (40%) and ‘confidence on self-knowledge’ (33%) among the medical students; whereas the main reason among non-medical students was ‘need immediate relief’ (24%) Nasir, et al. [6]. Antibiotic-resistant infections also contribute to the financial burden on health care systems Gelband, et al. [4]. Antibiotic prescribed by doctor group 13.57% know more about antibiotic resistance than self-medication 4.29%. The rate of self-medication with antibiotics (53.16%) is higher than the use of antibiotics prescribed by doctors (46.84%). Another study conducted on “Self-medication with antibiotics in Lithuania” in 2006 found higher prevalence of self-medication with antibiotics Berzanskyte, et al. [25]. It might be a global problem especially in developing countries Sallam, et al. [2].
Self-decision by previous experience/confidence was higher in age group 40-50 years. A study found that the parents who medicate their children do so in order to save money or to avoid a trip to doctor’s office Bennadi, [26-41]. Another study found that a number of reasons could be counted for self-medication such as strong desire of self-care, feeling of sympathy towards family members in sickness, previous experience of having antibiotic, lack of health services, saving money, ignorance, misbelieves, extensive advertisement and availability of drugs in other than drug shops are responsible for growing trend of self-medication and most importantly weak implementation of regulation related to medicines Oluyemi [8]. Most of the people (whom taken antibiotic as self-medication) were taken antibiotic due to Dysentery fever. Ciprocin, Metronidazole and Azithromycin, Cloxacillin and Amoxicillin were mostly used as 500mg dose. Daily frequency of taking antibiotics twice daily was most frequently practiced and the Ciprocin was highly practiced twice daily and secondly Azythromycin. Thrice daily was also most common for Metronidazole.Another study conducted in Bangladesh in 2014 also found that the highest percentage of self-medicated antibiotics was metronidazole (50.43%) followed by azithromycin (20.75%), ciprofloxacin (11.53%), amoxicillin (10.37%) and tetracycline (7.49%) respectively. The key reasons for the self-medication of antibiotics was the pre-experience (45.82%), suggestions from others (28.24%) and knowledgeable of the antibiotics (16.14%) Biswas, et al. [10].
There was strong association between the gender and antibiotic use and that is statistically significant (P-value = .024). The association between the income level and antibiotic use and that is statistically significant (P-value = .017). The association between the education level and antibiotic use and that is statistically significant (P-value = .002). There is strong association between the education and antibiotic users (self-medication and prescribed by doctor) and that is statistically highly significant (P-value = .000). Statistically there is no association. There was strong association between the income level and antibiotic user prescribed by doctor and that is statistically highly significant (P-value = .000). There was a strong relationship of antibiotics prescribed by doctor with income level. Income has an important effect on use of antibiotic practice (prescribed by doctor.
Conclusion
The practice of self-medication is higher in lower income andeducation level as these groups might have less knowledge about side effects and it is statistically significant also. The most common self-medicated antibiotics were Metronidazole, secondly Ciprofloxacin and thirdly Azythromycin. Antibiotics were selfmedicated mostly for the Dysentery, Fever, Common cold and Sore throat. Most of the participants’ source of antibiotics for selfmedication was private pharmacy and bought antibiotics from the pharmacy without prescription. Visiting pharmacy was the most common health seeking behavior among the participants who selfmedicated with antibiotics.
For more Articles on: https://biomedres01.blogspot.com/