Disabled Afghan Refugees in Iran: Beginning for the Future
Introduction
Afghan refugees’ population is estimated at over 950,000 in Iran [1,2] and most of them are living in urban areas [2] and out of camps [3] where are considered unsafe and poor environments [4]. It has been well known that delivering services are directly or indirectly affected by demographic characteristics of the refugees’ population [5,6], for example, the prevalence of chronic diseases can be higher in the older population [6]. On the other hand, providing services such as combined primary care and mental health have more obstacles when we are in contact with specific populations such as refugees [7] mostly as a result of differences in their attitude and believe [4]. Although as a result of the new registration system in Iran named Amayesh, more demographic characteristics and information has been collected [8] and few studies had performed on the health status of Afghan refugees in Iran [9] (as main purpose [4,5,10] or as a part [11-14] of those studies), there is, unfortunately, no accurate data and information regarding the prevalence of disability, its incidence and sociodemographic characteristics of disabled Afghan refugees in Iran. This may partly be because of the out-of-camp living of Afghan refugees in Iran [3] which makes data collection harder. The United Nations High Commissioner for Refugees (UNHCR) and The State Welfare Organization of Iran (SWO) are collaborating to provide rehabilitation services, assistive devices and equipment, and rehabilitation and treatment costs for disabled refugees in Iran [1,2]. Accessing that information will help SWO and other partners for better service deliveries and the sustainability of projects in the future. The main objective of our descriptive study is providing and obtaining sociodemographic characteristics of disabled Afghan refugees participating in a joint project of UNHCR and SWO in Golestan province, Iran between June until December 2015.
Materials and Methods
Data Collection
This study was a part of a joint project for disabled Afghan refugees in Iran between UNHCR, the Bureau for Aliens and Foreign Immigrants Affairs (BAFIA) of the Ministry of Interior of Iran, and SWO in 14 Provinces between June until December 2015 (project number: UNHCR 15/IRN/SWO/180). Golestan province is located in the northeast of Iran and for this project. we had 40 disabled Afghan refugees recruited based on information and profile of disabled Afghans in Gorgan city Welfare Administration. In total, there were 136 disabled Afghan refugees have been registered in the Golestan Welfare Administration. We included the first 40 individuals with a complete profile and passed a special commission to approve their disability type and its severity. During the project, two Afghan facilitators were trained by the province Welfare Organization to collect data and facilitate the delivery of rehabilitation services including individual and family education, assistive devices, medical follow-up, and providing basic needs.
Ethics Approval
Afghan refugees’ Information and data were used and analyzed by agreement of the Golestan Welfare Administration. All attention was paid to information confidentiality.
Statistical Analysis
The STATA SE v.12 (STATA Corporation, College Station, Texas) was used for analysis. We were cross-tabulated sociodemographic characteristics of the study population to calculate and present total and by sex prevalence.
Results
There were 40 individuals including 28 men with a mean age of 31.89 ± 18.07 (age range 8-72 years) and 12 women with a mean age of 19.67 ± 14.36 (age range 1-57 years). Most of the individuals (40.00 %) belong to the age group of 11-20 years old and single (72.50 %). Half of the sample lived in the urban area and 82.50% of them did not have any educations and were mostly unemployed (72.50 %). There was no individual with a university education. Almost all of the individuals lived in the rental house (95.00 %). There were not any individuals without a caretaker, but 75.00 % of them were cared for by one of the family members of which, 62.50 % of them were cared by their father and only 25 % were self-helped. Only 7 individuals had another disabled in their family (Table 1). In total, 42.50 % of individuals had Physical and motor disabilities. There were 42.50 % of individuals had a severe disability Table 2 showed information regarding disability types and severity among men and women. From 40 individuals, there were more men with physical and motor (35.71 %) and mental retardation (32.14 %) disabilities. Among 12 women, about 58% had physical and motor disabilities. In both sex, individuals with severe disability was more prevalent (men= 42.50 %, women= 50 %).
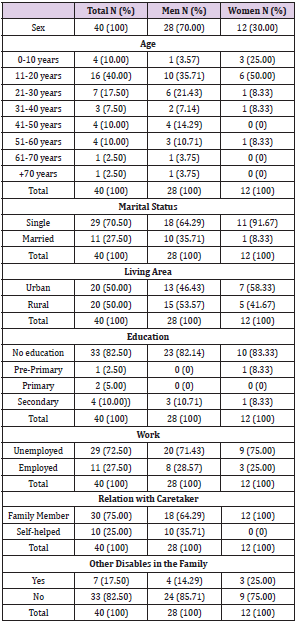
Table 1: Sociodemographic Characteristics.
Note: Results are presented as n (%) or mean ± standard deviation.
PCI: Percutaneous Coronary Intervention; CABG: Coronary Artery Bypass Graft; PAD: Peripheral Arterial Disease; CRF: Chronic Renal Failure; TIA: Transient Ischaemic Attack; CVI: Cerebrovascular Insult; CEA: Carotid Endarterectomy; CAS: Carotid Artery Stenting; CTA: Computer Tomographic Angiography.
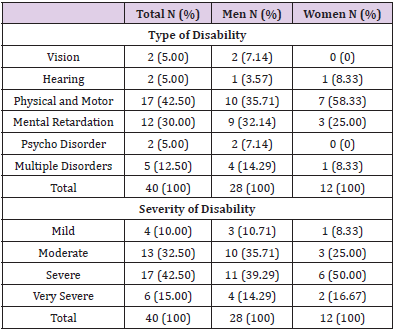
Table 2: Disability Characteristics.
At the beginning of this project, none of the individuals had healthcare insurance. But, during the project they could get the Salamat Health Insurance booklet (the universal public health coverage scheme in Iran) [1], therefore we did not show this information. Of 40 individuals, none of them had official training.
Discussion
Up to our search and knowledge, there were no published papers regarding disabled Afghan refugees’ status in Iran. This is a descriptive study as a part of a joint project between SWO, UNHCR, and BAFIA on disabled Afghan Refugees in Golestan province, Iran. There were 40 disabled Afghan refugees with mostly physical and motor disabilities who had received rehabilitation services and basic needs. Most of the individuals were without education and unemployed which can hinder any sustained empowerment of them. There are different partners with UNHCR for protecting, educating, health, and increasing the self-reliance of Afghan refugees in Iran [1,2]. This is a golden opportunity when Iran health system is faced with a high burden [4], so this capacity can be used to decrease the expenditure of the national health system [14], a succession of the international project, and the probability of the individual’s empowerment as an ultimate goal of the projects. Although only 12 women were in this project, we must consider cultural barriers, different attitudes, and being a refugee to participate in society [4]. In addition, service delivery for refugees living out of the camp is more difficult than residence in camps although they settled in urban areas and cities [6], and living space can affect individual’s health through their insight and type of relationship with those environments [15]. Although access to the number of health services such as family planning is the same for all individuals in Iran, the study showed lower usage by Afghans [4]. Therefore, programs and projects must-have elements and factors to integrating refugees into those societies besides providing rehabilitation, treatment costs, assistive devices, and environment adjustments.
Having one family member as a caretaker, although can reduce disability side effects and can lead to low family income especially when a father or mother with older ages becomes a caretaker and there might be an ambiguous future for them after losing their caretaker. This can also, besides low socioeconomic status, unemployment, and low grades of education may increase food insecurity [16] which may aggravate disability. Therefore, having an insurance system that covers both treatment and rehabilitation costs and pension payments can help them to have a better quality of life. Comprehensive health insurance would be one way for lowering out-of-pocket payments for using rehabilitation and health care services when it is almost the same as other citizens’ insurance. Health insurance in itself may not guarantee better access to health services for refugees. Since this coverage is at the very beginning steps, studies must be carried (both qualitative and quantitative) to discover accessibility, advantages, disadvantages, barriers, and the attitudes of refugees using services. Iran’s government has started to repatriate Afghan refugees but on the other hand, education, medical treatments, work, and economy have been reported as the main concerns of refugees to return to Afghanistan [8]. This situation may become more prominent for disabled refugees. Therefore, more comprehensive planes and dedicated projects to empower refugees are needed to facilitate repatriation. Changing trends from no education for girls towards educating them at any costs, as a result of staying in Iran during the past years, can be used as an opportunity for a succession of educational projects [8], although most of our disabled refugees remained without education. A program such as family planning and reproductive health was successful in the Afghan refugee society through shifting attitudes and beliefs [3] which indicates the possibility of making changes among them to achieve disability prevention.
Limitations and Strengths
The main limitations were the unwillingness of refugees and their families to participate and attend in disability assessment commissions and projects in addition to difficulties to have accurate information when asking sensitive questions such as housing and employment status. We were not able to collect income information of refugees since they did not have regular and monthly paid jobs. These limits may be partially or completely due to fear of returning to Afghanistan [16]. Although we had training sessions for our facilitators, a longer period of education with more materials would increase their competence. Inability to have and involve undocumented disabled refugees [17] in this and similar projects was another problem since they live in the society, not in camps. As a strength, we used Afghan facilitators to make better trust and tackle the language and ethnic barriers.
Conclusion
Although joint programs are comprehensive and may lead to better service delivery to those marginalized groups including refugees, cooperating organizations and sectors need to be in line with the goals of those programs.
For more Articles on: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.