Assessment of Bone Strength in Atrophic Edentulous Mandible by Using Finite Element Method
Introduction
Recently, the elderly’s quality of life has been emphasized with the prolongation of the average life span. The act of taking meals through the mouth is an important factor even in a longevity society. On the other hand, in the elderly, the incidence of oral problems has increased, and an edentulous jaw requiring a denture is a representative one. Marked atrophy of the mandible is noted in elderly persons requiring a denture; bone strength is limited. In this study, we investigated the pattern of fracture in accordance with mandibular loads with respect to the presence or absence of denture wearing in a patient with atrophy of the edentulous mandible.
Materials and Methods
We performed finite element analysis in a 71-year-old female with an edentulous mandible. Using the Digital Imaging and Communications in Medicine (DICOM) data obtained on computed tomography in this patient as the material, the edentulous mandible was extracted, and a three-dimensional model was prepared using a personal computer. Using this model, a bruise on the mentum of a denture-free or -wearing edentulous mandible was reproduced (Figure 1). For the finite element analysis/evaluation, we used software for finite element analysis, Mechanical Finder (Research Center of Computational Mechanics, Inc., Tokyo). As the material properties of the mandible, we used the material property value calculated from the CT value based on Keyak’s formula (A Poisson’s ratio of 0.4 was used). For fracture reproduction, loading/constraint conditions were established so that a mental bruise might be reproduced, assuming a status of a falling-related bruise on the mentum. Loading conditions were established at the mentum. Constraint conditions were established at the jaw-assumed condylar process/mandibular head and denture-wearing-assumed alveolar parts of the mandibular midline and body. However, when establishing the constraint conditions for the mandibular head, one node of the mandibular head was completely constrained, and the other one was constrained in directions other than the X-direction (Figure 2).
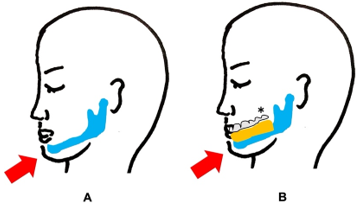
Figure 1:
A. Edentulous mandible without a denture,
B. Edentulous mandible with a denture. An arrow at the mentum indicates an external force. (*; denture)
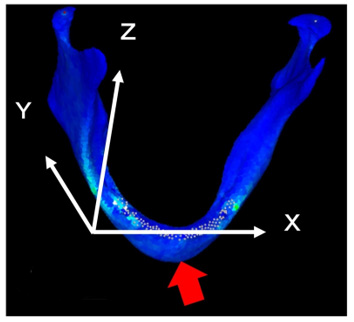
Figure 2: A 3D mandible model from an edentulous jaw patient. The x-, y-, and z-axes were established, as shown in this figure. The mentum was loaded (red arrow).
Results
The primary sites of bone destruction were the mandibular head and body. In denture-free patients, destruction of the mandibular head initially occurred under a load of 300N. When the load was further increased, destruction of the mandibular body occurred under a load of 1,200N. In denture-wearing patients, destruction of the mandibular body initially occurred when adding a load of up to 900N. When the load was further increased to 2,400N, destruction of the mandibular head occurred (Figure 3).
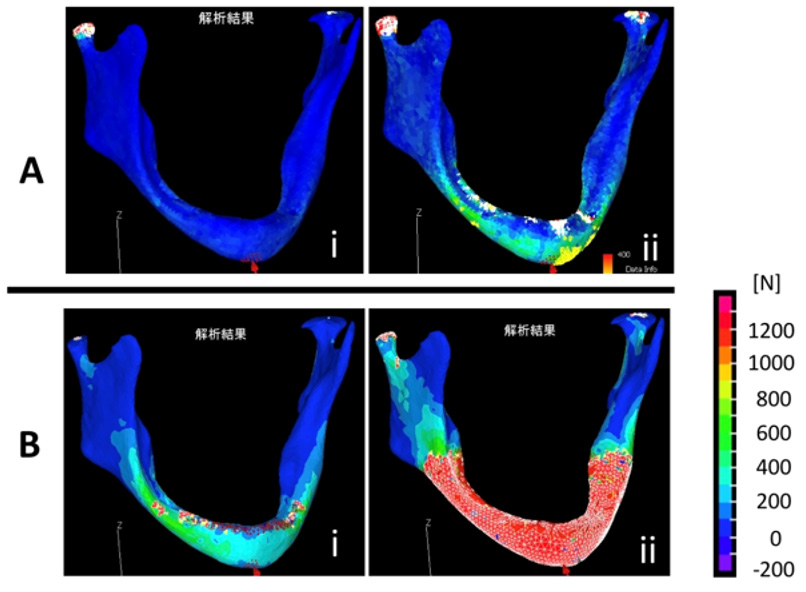
Figure 3: Bone strength of atrophic mandible examined by finite element simulation analysis. Bone strength was measured by finite element simulation analysis after applying a mechanical force to mental part. Red indicates the areas of compression fracture, and white indicates the areas of tensile fracture.
A. Edentulous mandible without a denture.
i) Destruction of the mandibular head occurred under a load of 300N.
ii) Destruction of the mandibular body occurred under a load of 1,200N.
B. Edentulous mandible with a denture.
i) Destruction of the mandibular body occurred under a load of 900N.
ii) Destruction of the mandibular head occurred under a load of 2,400N.
Discussion
The improvement of life environments has prolonged the average life span, increasing the number of elderly persons. As a result, the incidence of aging-related diseases, such as atrophic fracture of the mandible, has increased [1]. The risk of fracture depends on the degree of atrophy of the mandible. It is high when the height of the mandible is ≤20 mm [2]. When atrophic fracture of the mandible occurs, Open Reduction and Internal Fixation (ORIF) is the gold standard treatment method. However, mandibular reconstruction with a free fibula flap is recommended in accordance with the patients [3]. Of patients with fracture of the mandible, 3% had an edentulous mandible. In these patients, various treatment methods, such as sprints, dentures, intra-bone wire fixation, and fixation with mini plates and screws, were used [4]. However, the incidence of complications after reduction in patients with an edentulous mandible is reportedly 18% [4]. In our institution, for the treatment of atrophic edentulous mandible fracture, surgical approaches or fixation methods are also selected/determined through a sufficient review, and follow-up is conducted, considering postoperative denture wearing. In any case, it is difficult for health care professionals to select or determine treatment methods in many patients with atrophic edentulous mandible fracture.
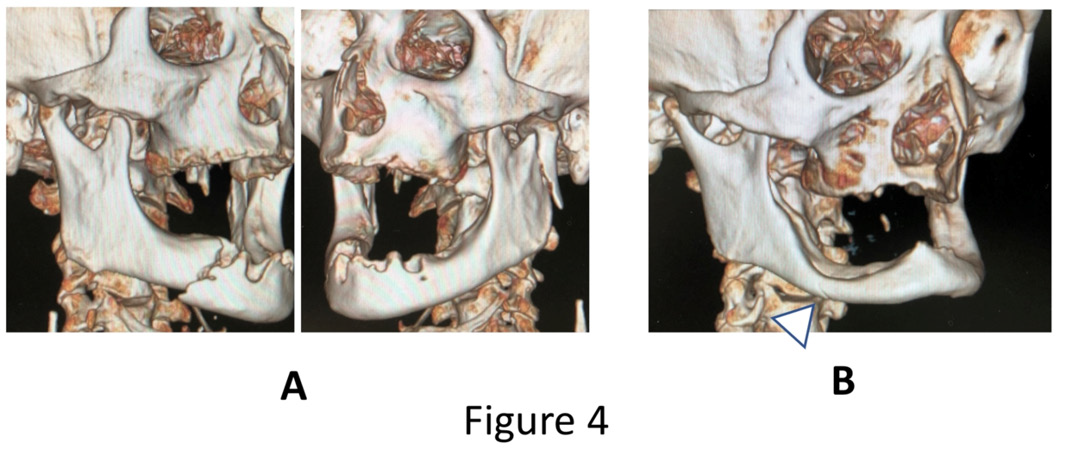
Figure 4: Case presentation
A. A 74-year-old male. Falling in a denture-free state led to a bruise on the mentum. Fracture of the right mandibular body and left mandibular head was observed.
B. A 71-year-old male. He was injured due to high-energy trauma, that is, traffic trauma, under denture wearing. Fracture of the right mandibular body was noted (arrow).
In this study, fracture of the mandibular body and head was reproduced through simulation. Previous clinical reports also indicated that the frequent sites of atrophic fracture of the edentulous mandible included the mandibular body and head [5]. A representative case of fracture of the edentulous mandible is shown in Figure 4A. In this denture-free patient, fracture of the right mandibular body and left mandibular head occurred despite injury related to a relatively small external force associated with falling. In another denture-wearing patient (Figure 4B), traffic trauma, that is, injury related to a relatively large external force, was noted. However, fracture involved the mandibular body alone. Through this finite element analysis, we clarified that the mode of fracture depended on the presence or absence of a denture in patients with atrophic edentulous mandible. As presented in Figure 4, a weaker force may induce fracture in the absence of a denture, and fracture of the mandibular head, which is more difficult to treat, may occur. In contrast, a greater force is required to induce fracture in denturewearing patients; therefore, denture wearing may reduce the risk of bruise-related fracture. In addition, even when fracture occurs, it initially involves the mandibular body under a small impact; therefore, treatment may be easier than mandibular head surgery.
Conclusion
In patients with an edentulous mandible, fracture of the mandibular body and head was frequent, and there was a certain tendency to the frequent site of fracture with respect to the presence or absence of denture wearing. It is important for patients with atrophic edentulous mandible to understand the risk of fracture. Denture wearing at all times may more markedly reduce the risk of fracture on bruises.




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.