Takotsubo Cardiomyopathy After 3rd Dose of mRNA COVID-19 Vaccination: A Case Report
Case Report
A 90-year-old woman with past medical history of hypertension, hyperlipidemia, chronic kidney disease and post transcatheter aortic valve replacement (TAVR). She was admitted to the emergency department due to sudden onset of dyspnea which started 1 day after receiving the third dose of BNT162b2 mRNA Pfizer vaccine, she had no chest pain, palpitations, cough or fever. She reported no symptoms after her second dose of the vaccine which she received 6 months prior to the third dose. On presentation she was hypoxic with 79% on room airand diffuse lung crepitations on auscultation, heart sounds were normal with holosystolic murmur consistent with mitral regurgitation. A chest x-ray showed pulmonary edema. Initial laboratory tests revealed elevated levels of high-sensitivity troponin I at 186 ng/L (n <6 ng/L) which further peaked to 9415 ng/L in the next 12 hours. An ECG showed mild ST segment elevation in leads V2-4 (Figure 1). Invasive coronary angiography ruled out obstructive coronary artery disease (Figure 2). Transthoracic echocardiogram showed apical ballooning (Figure 3) with estimated left ventricular ejection fraction of 35-39%. TC was further confirmed by cardiac magnetic resonance imaging (CMR) that showed edema in mid-apical region with increased relaxation time from basal to apical level (Figure 4). The patient showed good improvement and recovery in her clinical condition and was discharged in a stable condition.
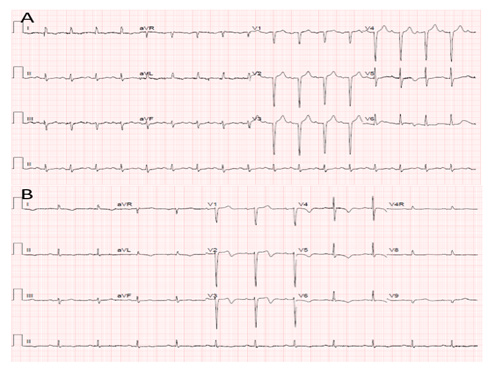
Figure 1:
A. ECG recording at presentation which showing LVH with Q waves in anterior leads.
B. ECG recording at the third day of hospitalization showing inverted symmetrical T-waves in all precordial leads.

Figure 2:
A) Right coronary artery without evidence of obstructive lesions.
B) left coronary artery without evidence of obstructive lesion in any segment.
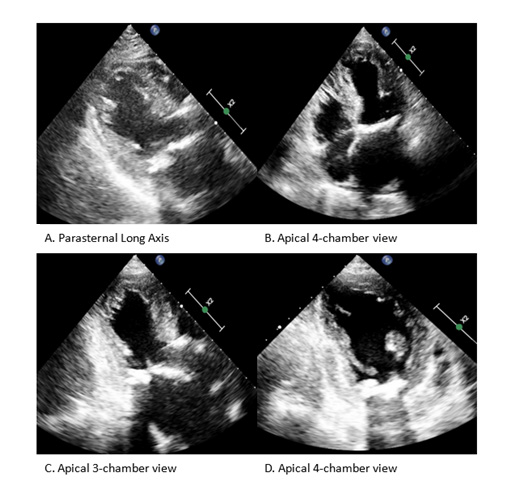
Figure 3: Transthoracic echocardiogram showing apical ballooning.
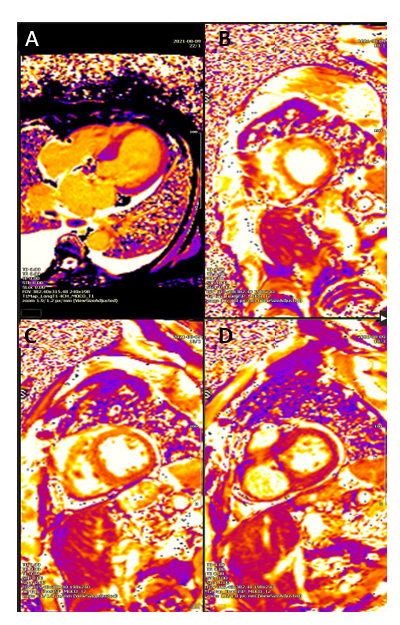
Figure 4: Cardiac Magnetic Resonance – Native T1 mapping showing increasing relaxation time from base to apex.
(A) Long view
(B) Apex-level
(C) Mid-level
(D) Basal level.
Discussion
To the best of our knowledge, this the first case to describe TC following the 3rd dose of vaccination for COVID-19. This highlights a rare but serious cardiovascular event occurring shortly after COVID-19 vaccination. Previous reports suggested an association of the second dose of mRNA-1273 SARS-CoV-2 vaccine [3] and after influenza vaccination with TC [4,5]. The third dose of mRNA vaccine (COVID-19 vaccine booster) is the new strategy in to cope with the COVID-19 pandemic. While healthcare professionals are encouraging the population to receive the booster vaccine in hope that a critical mass of vaccinations could avert a national lockdown to stem the spread of the ultra-contagious new variants of the coronavirus, it will be important to follow-up these unusual events to better understand the reactions to COVID-19 3rd vaccination.




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.