Easier Left Sided Bronchial Blocker Placement Using Middle Fixation of Endotracheal Tube and Real Time Wireless Video Fiberoptic Bronchoscopy
Editorial
In our institute, Dr. Cherng’s article: “Middle fixation of electromyographic endotracheal tube for intraoperative recurrent laryngeal nerve monitoring“ [1], they described that electromyographic endotracheal tube (ETT) should be affixed at the middle of the mouth to avoid missing contact with one side vocal cord. However, we’d like to share our experience of using middle fixation of the EET and real-time wireless video fiberoptic bronchoscopy for facilitating left‐sided bronchial blocker (BB) placement. BB products typically have been deployed within the ETT or intraluminally after intubation for one lung ventilation [2]. However, intraluminal placement of these devices sometimes can be challenging, with both the blocker and flexible fiberoptic bronchoscope (FOB) present within the ETT, especially the left-sided BB placement [3,4].
Moreover, the angle of tracheobronchial relationship favored the preferential passage of the right-side BB placement [4]. Therefore, in order to increase the success rate of left-sided BB placement, the extraluminal placement technique and using the preshaped Fogarty catheter as a bronchial blocker have been developed [4,5]. But the extraluminal placement technique is prone to sorethroat or hoarseness, and the success rate of preshaped Fogarty catheter to the left bronchus is low (18.2%; 2/11) [3,4]. Here, we introduce a new method to make left-sided BB placement easier by using middle fixation of EET and real-time wireless video fiberoptic bronchoscopy. After tracheal intubation with a EET (I.D. 7.0 mm for women and 7.5 mm for men), we kept the EET affixed between incisors, at the middle of the mouth (Figure 1) and the distal ETT within 2-5 cm above the carina to improve the visual field , because tube rotation and deviation may occur when the ETT is affixed at the right or left mouth corner [1,6]. Then, a BB (Coopdech endobronchial blocker tube, Daiken Medical Corp., Osaka, Japan) was advanced through the blocker port of its special multiport connector and the 2.8 mm FKScope (WD-OD28-160K-47-A1, Johnfk Medical Inc., New Taipei City, Taiwan), a real-time wireless video fiberoptic bronchoscopy, that had been introduced through the fibreoptic port. And the blocker is advanced with a counterclock twisting motion to direct it into the left main bronchus under the FKScope . Finally, the blue balloon of the BB was inflated and the correct position was confirmed with the FKScope (Figure 2) and auscultation.

Figure 1: The endotracheal tube is affixed between incisors, at the middle of the mouth.
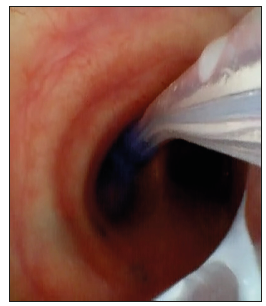
Figure 2: Place the bronchial blocker into the left main bronchus by using wireless video fiberoptic bronchoscopy.
Evidence of Genomic Damage Induced By Prodigiosin Produced By Serratia Marcenscens Ufpeda 395 in Human Peripheral Blood Mononuclear Cells-https://biomedres01.blogspot.com/2021/01/evidence-of-genomic-damage-induced-by.html
More BJSTR Articles : https://biomedres01.blogspot.com




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.