Educational Intervention for the Prevention of Sexually Transmitted Infections in Seventh Grade Adolescents
Introduction
Adolescence is a stage in which social interests appear and
feelings never before experienced blossom, which together with
physiological changes make evident a significant transformation
in this subject that little by little ceases to be a child [1]. It is an
era of continuous biopsychosocial changes, where the aim is
to strengthen the personality and the roles that will develop in
society. It is considered a period of human development in which
an important decision-making process of the subject begins with
respect to itself; it is also the beginning of the transition towards
adulthood. The adolescent often faces, without possessing the
necessary psychological resources to the problem of starting to
outline the ways to follow to fully incorporate into society, so that
his projection of life and his position within it change [2].
This is also a formative stage, crucial in the life cycle; identity, autonomy and the project of life are being conformed, reason why an integral approach of the sexuality is necessary, taking into account that the influence exerted of the different spaces where the adolescents develop in their daily life is determinant, if considers that at this stage of life, relationships with their peers are very significant [3,4]. With regard to the relationship of couple begins to relegate friendship relations to the background. Relationships at this stage tend to be unstable, since they have an experimental nature and contribute to the development of the self-assessment or personal identity and, in particular, the sexual and gender identity of the adolescent [5-7].
One of the fundamental aspects in these ages is sex, indissolubly linked to the human being as a biological entity; it is a natural instinctive process, modified by social patterns. This stage should be one of full enjoyment and for this purpose, adequate orientation is necessary [8]. Adolescents do not count (in many cases) with an adequate sex education, so they constitute a risk group par excellence for contracting sexually transmitted diseases and they can also reach early motherhood or fatherhood for which they are neither objective nor Subjectively prepared [7]. In the choice of the couple the adolescents have difficulties to make coincide their ideal -from the physical point of view- with the ideal to which they aspire according to their psychological and moral qualities, due to the great importance that they give to the corporal image. In adolescence, the stereotypes corresponding to the male and female sex roles are polarized in a particularly abrupt manner, and the need to correspond with them becomes more acute than ever [5,6].
In men - more than in females - sexual maturity anticipates the development of the resources necessary to establish a relationship in which stability, psychological intimacy and mutual understanding are achieved [7].
The females, also attending to the stereotypes linked to their gender role, are more free to give themselves from the affective in the couple’s relationship and, at the same time, taking into account what is expected in their sexual role, they must hide their feelings, since “wait” and “take their place” are qualities that are linked to values such as feminine dignity and reputation. This separation between what is erotic-sensual and tender depends, to a large extent, on macho prejudices, according to which the traditional style of masculinity and virility are legitimized by the approach of man to woman from positions of strength [6,7]. Therefore, the health of adolescents could be at risk due to inappropriate sexual and social behavior. The combination of both is frequent and very dangerous for sexual and reproductive health [9]. The main consequence of sexual risk behavior is framed in the reproductive damage with presence in the increase of Sexually Transmitted Infections [3]. Statistics worldwide estimate that in 2015 1.2 million adolescents died, that is, more than 3000 a day, mostly due to preventable or treatable causes [10].
New HIV infections among children have decreased by 58% since 2001 however it is reported that in 2013, 240,000 children were infected by the virus. AIDS is today the leading cause of death among adolescents (10 to 19 years old) in Africa and the second most common among adolescents worldwide. One million pregnant women get infected every year with syphilis. In 2012, Syphilis affected 360,000 pregnancies [11]. In Cuba, the average age of onset of sexual intercourse is increasingly low; The earlier the first intercourse occurs, the greater are the risks of pregnancy and of contracting sexually transmitted diseases [12]. This demands greater actions aimed at protecting adolescents in terms of sexuality, since it is a universal right of all people in relation to the full, healthy and free enjoyment of all discrimination and social injustice.
Methods
Type of Research
study of educational intervention quasi-experimental pre-post test with quantum-quantitative control group in adolescents of the Basic Secondary School “Antonio José Oviedo” of the municipality of San José de las Lajas, during the school year from doctors previously trained for the study in question. Methodologies were applied for the prevention of STIs-HIV / AIDS in adolescents and young people in the school setting [12-15]. The study universe consisted of 150 7th grade students. Shows 60 students selected by the simple random method. It was conditioned by the requirements of the activity according to the number of participants, the goals and pedagogical methods to be used.
Inclusion Criteria
a) 7th grade students with ages between 12 and 13 years old, belonging to the Basic Secondary School “Antonio José Oviedo”
b) Approval of parents and students to participate in the study.
Exclusion Criteria
a) Students who were absent from 3 sessions.
5. Techniques and Procedures
The Investigation was Divided into Three Stages
Diagnostic Stage: The introduction to the educational program was made, where the work was made known. The survey was applied to the students in order to specify the degree of information they have about STIs, prior to the educational intervention. The survey model was the informative support of the work; It allowed to collect all the variables of interest, such as: sociodemographic, of sexual activity, knowledge of STIs-HIV / AIDS, complications, beliefs about these, knowledge about the condom, perception of risk and attitude toward people infected by STIs. He was asked for his written approval to be included in it.
Intervention Stage: The results of the initial questionnaire were analyzed, and the educational strategy was designed. There were 15 work sessions in the form of workshops with a weekly frequency and a duration of 45 minutes, for 6 months. During the sessions, knowledge of the most frequent STIs, predominant manifestations, transmission routes, complications related to them was deepened, correct condom use was emphasized, values such as companionship, altruism were strengthened, myths and erroneous beliefs were demolished. STI-HIV / AIDS and condoms, the fields of vision were expanded close to the perception of risk and sexual risk behaviors for the acquisition of STIs in general. Participatory techniques were used with the aim of achieving the participation, animation and integration of the participants and making the understanding of these issues easier, as well as favoring reflection.
Evaluation Stage: It was done six weeks later, where the initial survey was applied again. In this way, the evaluation that was carried out before and after the intervention stage made it possible to assess the changes produced in the knowledge, which were considered as the effect or result of the educational tasks carried out with the adolescents. The results are presented in the form of tables for better understanding.
Operationalization of the Variables
Ethical Aspects
communication to the scientific council of the institution. No disclosure and confidentiality of the student’s name. The data will only be used for scientific purposes.
Processing of Information
The information was obtained from the results of the questionnaire created by the INHE-M [14]. The processing was done in the Microsoft Excel Office 2007 database, the data was collected in an emptying sheet using the Excel program of the Office, which allowed expressing the information by means of the descriptive percentage statistics and for the inferential statistics the Chi square was used through the epidemiological analysis of tabulated data (EPIDAT version 3.1) (Table 1). The results were subjected to analysis and discussion, comparing them with the results described in the literature by other authors, based on an inductive and deductive analysis, reaching conclusions and making recommendations aimed at establishing a group of actions aimed at increasing knowledge about about STIs-HIV / AIDS in the study group. The qualitative component was related to the social aspects that aimed to understand certain behaviors, attitudes and how the adolescents have been affected by events that happened around them (Table 2). The subjective reality that allowed the interpretive richness and contextualized the phenomenon by expanding the investigation was analyzed [16]. The quantitative study was carried out by quasi-experimental study before and after where the data were collected through an instrument created for this purpose, measuring the phenomenon with the use of statistical methods, this allowed objectively to analyze reality [16].
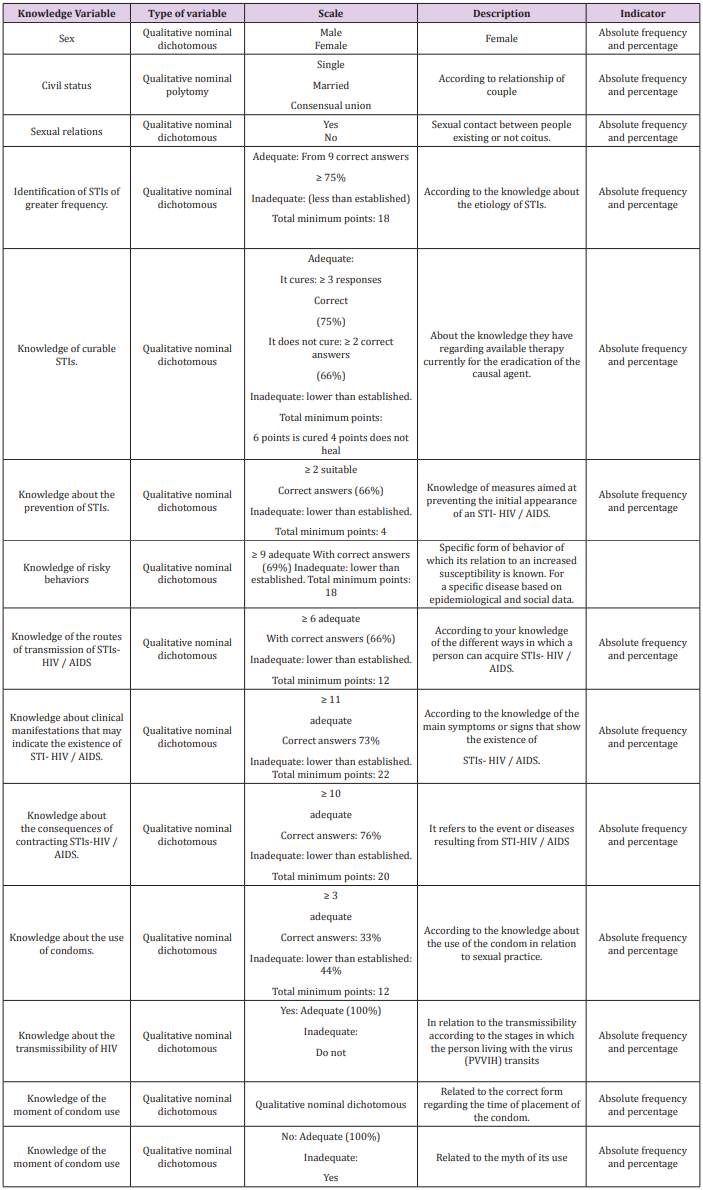
Table 1: Excel program of the Office, which allowed expressing the information by means of the descriptive percentage statistics and for the inferential statistics the Chi square was used through the epidemiological analysis of tabulated data (EPIDAT version 3.1).
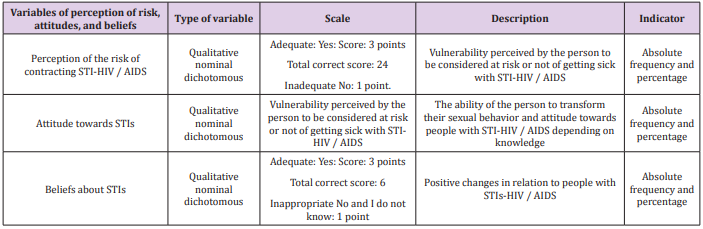
Table 2: The adolescents have been affected by events that happened around them.
Results
It is observed that 33 students belonged to the female sex and that the highest percentage belongs to single marital status calling attention to the fact that 4 students declared having stable relationships with consensual or married union. It was observed that 23 students had had sexual relations for 38% of the total and of them the females present the highest percentage (44%), which was statistically significant (p = 0,2272). The results of the responses considered adequate before and after the educational intervention on STI / HIV-AIDS are shown. It is observed that there is an increase in the variables of knowledge, perception of risk and attitude, reaching 93, 90, 73% post intervention respectively, beliefs rose from 26 to 86%, it was statistically significant.
In the case of the results obtained in the control group on the level of knowledge, risk perception, attitudes and beliefs, it is observed that there were no significant results according to the established standards, but that the inadequate responses continue prevailing.
During the present investigation it was possible to establish the relationship between some questions of the applied questionnaire. There is an association between the risk of contracting HIV / AIDS when having sex with known people and there is no concern about this probability with low percentage in the pre-test. After the intervention it was possible to increase the perception of risk of the majority of students in 86-100%. It was also found that at the beginning of the study most of the students did not consider that they could be exposed to HIV / AIDS in the first sexual relationship, nor did most of them wonder if their partner could have the virus (10 and 23%) respectively. After the educational intervention rises significantly, it was achieved that 83 and 96% raised their perception of risk in both cases respectively (Tables 3-8).
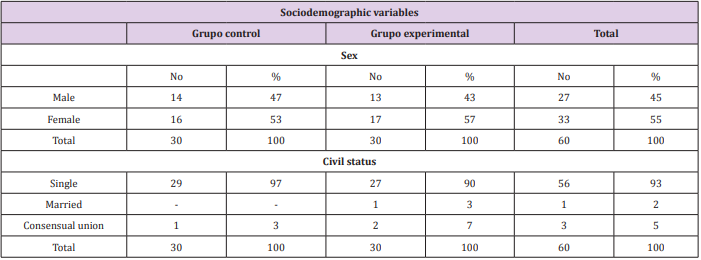
Table 3: Sociodemographic distribution of the students of the experimental group and the control group.
Note: Basic Secondary Antonio José Oviedo

Table 4: Distribution of adolescents according to sex and sexual relations. Experimental group and control. Basic Secondary Antonio José Oviedo.
Note: p= 0,2272

Table 5: Behavior of variables under study in the experimental group.
Note: p=0.000

Table 6: Behavior of the variables under study in the control group.
Note: (p=0.000)

Table 7: Relationship between the perception of risk of contracting HIV / AIDS with well-known people and the question of whether it will be a carrier of the virus. Experimental group.
Note: p= 0,1732

Table 8: Relationship between perception questions: being exposed to AIDS in the first sexual relationship and the possibility that the couple may be infected or sick. Experimental group.
Note: P=0,3400
Discussion
After showing the results, the predominance of the female sex was appreciated, not coinciding with studies of the socio-demographic characteristics of the adolescent population in Cuba where male adolescents (689 867, 51.50%) over female (649 468) predominate very discreetly. 48.49%) [12]. It is also evident that although most of them were single, we can not forget that 4 students were with a stable union, either married or consensual free union, and that 23 students declared having presented sexual relations at some point, corresponding also with greater percent to the female sex. It coincides with other studies on this topic. According to the results of the 2014 MICS, 15.8% of women between 15 and 19 years of age, were married or in union (16%), 31.2% of those under 18 had been married in marriage at least once and 5.9% before the age of 15. 12.9% of women under fifteen years old reported having had sexual relations [17]. STIs have increased their incidence of gonorrhea, syphilis and condylomas among Cuban adolescents and youngsters. This is a worrisome situation. After observing the results, before the educational intervention, the students had a low level of knowledge about STIs / HIV-AIDS. Most of them initially did not know how to identify the different types of existing infections, whether they are curable or not, the routes of transmission, clinical manifestations and possible complications. With respect to the use of condoms, they did not identify well when it was the sexual act to place it or if it was safer to use two at the same time. These inadequate knowledge then lead to the appearance of STIs at an early age [17-19].
The authors consider that the low perception of risk presented by adolescents is clear, considering that knowing “well” a person, or being their first sexual relationship is not exposed to AIDS or other STIs, which is a great mistake, As it is well known, “AIDS does not have a face”, a phrase that is frequently repeated in the audiovisual and folding promotion media. This situation is due to the fact that adolescents are not biopsychosocially prepared to initiate sexual relations, in this case evidenced by the seventh grade students of the research who are still in an early adolescence and this affirmation is in agreement with other authors [20-25]. In the case of attitudes and beliefs initially they were also reflected in an inadequate way. Attitudes although after the intervention showed better results we ratify that they are more complex in their process since they need interventions of greater durability in time to take their modifications as true and significant. Since the fact that a person acquires a certain level of knowledge does not mean that they change their attitude towards dealing with HIV-positive persons, although in Cuban society solidarity and humanism prevail as general distinctive characters [26].
Although before the intervention we found that the variables were unsatisfactory, we now propose that the expected results were obtained, coinciding with other educational interventions already carried out, where up to 79% and 85% of satisfactory results were achieved [26-25]. When comparing the data obtained with the empirical investigations carried out after the intervention, it can be seen that the results are in tune with the current trends in the effectiveness of the interventions, with the one proposed by this research being one of the most satisfactory and significant results [26-31]. The economic valuation and the social contribution are evident in that these results affect not only the individual welfare but social, with the decrease of these infections from an early age, the risk of infection is reduced and with it the excessive use of medicines that cost so much result for the Cuban economy [32].
Conclusion
a) There was a low level of knowledge about STIs / HIV-AIDS in seventh grade adolescents despite receiving such topics as part of their curricular educational pre-intervention program. The application of the questionnaire collected information on different variables that allowed the analysis of the adolescent as being biopsychosocial.
b) There was an increase in adolescents’ knowledge about STI / HIV-AIDS post-intervention as well as the perception of risk, attitudes and beliefs.
c) The implementation of educational methodology in
adolescents was effective in raising the level of knowledge, risk
perception, attitudes and beliefs about STIs / HIV-AIDS.




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.