Diagnostic Significance of Fine Needle Biopsy and Cell Block in Skin and Subcutaneous Nodules
Introduction
Skin and subcutaneous lesions are a common reason for
patients to visit family doctors. Ultrasound is increasingly being
used to confirm the diagnosis, but deep lesions must be evaluated
with magnetic resonance imaging (MRI) or computed tomography
(CT) to exclude invasion of the underlying structures and/or
malignancy [1]. People can experience a wide range of growths and skin
changes over the course of their lives. Family physicians must
be able to distinguish between different skin tumors specially to
rule out malignancy [2]. Skin malignancy represents one of the most
dangerous types of cancers. It spreads gradually in its early stages,
so it is necessary to detect it as soon as possible. It is suggested
that skin cancer results from the presence of unpaired strands
of deoxyribonucleic acid (DNA) in skin cells, resulting in skin
genetic defects or mutations [3]. Evaluation of patients with skin
or subcutaneous nodules, especially if they are multiple, is a major
problem for clinicians. But with full investigations, the problem
becomes easier. However, the definitive diagnosis depends on the
pathological reports of tissue biopsy [4]. Easy access to skin nodules
provides a good platform for performing fine needle cytology and
sampling by pathologists or clinicians. Smear cytology gives several
default settings [5]. Depth is more important than width. The skin
nodule may be mobile or fixed in the underlying tissue. Proper
management of skin or subcutaneous nodules needs to know their
exact nature, benign or malignant. These nodules can be accessed
through needle aspiration, to make smears and cell blocks; this
action is relatively non-invasive outpatient procedure and does not
require an operating room or anesthesia. It is also a cheap and fast
process. Furthermore, it has been suggested that FNAC breast exam
is very useful, relatively quick, inexpensive and less invasive test
due to the size of the fine needle, and is easier and safer in some
lesions, such as very small lesions or those directly under the skin
[6]. The question was how is his sensitivity and specificity, and to
what extent can he be relied upon in making a treatment decision?
Therefore, this study aimed to verify the reliability of examination
of smears and cell masses in the diagnosis of skin and subcutaneous
nodules and to compare them with examination of tissue biopsies.
Material and Methods
Study Design and Samples’ Preparation
Samples of cutaneous or subcutaneous nodules from two hundred and twenty-five patients who decided and gave written consent to participate in the study were selected for this study. These patients were referred from various related clinics in University Hospitals to the Department of Pathology between January 2018 and December 2020. The patients underwent full history taking, general examination for pulse, temperature, respiration rate, body weight, and height. All malignant nodules were primary lesions. The nodules under study were examined clinically for location, size, plurality, shape, consistency, color, if hair was present or not, and whether there was change in color, size, shape, mobility or fixation. Then, a sterile 10 cc plastic syringe was opened, approximately 1 cc of air was taken, the cover was placed on the needle and it was ready for use. The lesion and the surrounding skin underwent a gentle massage with cotton gauze filled with 95% ethanol, then the needle was inserted close to the periphery of the node (avoiding the center where there may be necrotic material that hinders proper smear taking). The needle was moved in multiple directions with suction; then it was gently removed. Then, the suction site was under pressure with clean, sterile cotton gauze for at least 10 minutes to stop possible bleeding. The needle was gently removed from the syringe, and then 1 drop of the syringe’s content was placed on approximately 4 clean glass slides. The smear was prepared by gently moving the blunt end of the syringe.
The remainder of the fluid underwent addition of a mixture of10% neutral buffered formalin, and absolute ethanol, 1:1 solution by gentle suction of the previously prepared formalin/ ethanol mixture by the syringe. The smear was allowed to dry on the glass slides, then the slides are placed vertically in the staining container, with the addition of 95% ethanol, and left for 20 minutes to fix. Fixed smear slides were gently placed in water for 1 min, then in filtered hematoxylin for 5 min, then in tap water for 30 min, then in eosin for 1 min in tap water for 20 min. The slide smear then, underwent placing in ascending grades of ethanol till absolute alcohol. A cap was placed on the smear, which was then examined with an Olympus XL 30 binuclear microscope. The pellets of cells in the used syringe, were left for one day for fixation, then underwent processing to form paraffin blocks, according to Hegazy Method of tissue processing [7]. Unstained slides were prepared from the paraffin blocks then staining with Hematoxylin & eosin (H&E), Giemsa stain and Papaneacolou stain (PAP). Then, the slides were examined with an Olympus XL30 binuclear microscope and photographed with the digital camera on the microscope. Patients in this study underwent FNAC smears, performing cell masses if possible. Then, histological examinations of tissue biopsies were performed after surgical removal of the lesions.
Statistical Analysis
The correlation between results of FNAC smear and that of cell block study was examined by chi-square test and student T-test. Sensitivity test, & Specificity test for both FNAC smear and cell blocks were examined in relation to the tissue biopsy, considering the results of tissue biopsy examination as the reference positive cases [8]. All statistical tests were done with considering the significance value of chi-square test and T-test (P value significance =0.05 or less) using SPSS 16.0 for Windows (SPSS Inc. Chicago, Illinois, USA)
Results
There was a wide range of ages in the patients who underwent
this study. Their ages ranged between 2 and 76 years but most of
them (80%) were between 40-45 years old. The genders of patients
were predominantly female. The female to male ratio was 3 to 2,
respectively. The results of the FNAC smear, cell block examination,
and tissue biopsy examination are presented in Tables 1-3. The most relevant pictures of microscopic examination are placed in
(Figures 1-10). Sensitivity and specificity test results of both FNAC
smear and Cell block examination are summarized in the following
data:
For the FNAC smear examination:
True positive cases = 220/225.
True negative cases = 5 /225.
False positive cases =25/225.
False negative cases = 45/225.
Sensitivity test = 220/220+45= 220/265=83.01%.
Specificity test = 5/5+25=5/30= 16.66%.
For the cell blocks examination:
True positive cases = 220/225.
True negative cases = 5 /225.
False positive cases = 0/225.
False negative cases =5/225.
Sensitivity test = 220/220+5 =220/225 =97.77%.
Specificity test = 5/5+0=5/5 = 100%.
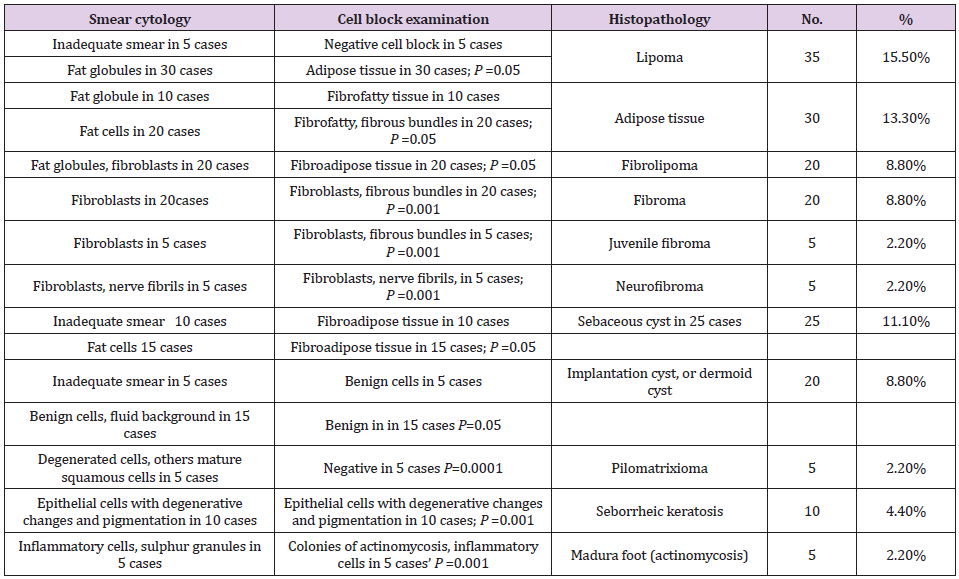
Table 1: Results of FNAC smear, cell block examination, tissue biopsy in the benign nodules.

Table 2: Results of FNAC smear, cell block examination, tissue biopsy in the benign nodules.

Table 3: Results of FNAC smear, cell blocks, and tissue biopsy in malignant nodules.
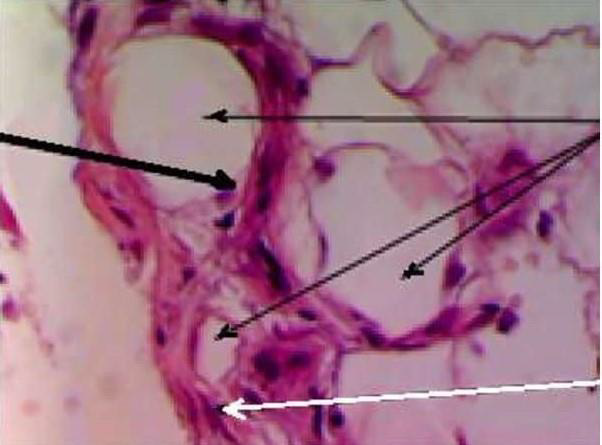
Figure 1: Cell block from a case of fibrolipoma showing mature fat cells (thick arrow), fat globules (thin arrows), fibroblasts and collagen bundles (white arrow). (H&E, x400).
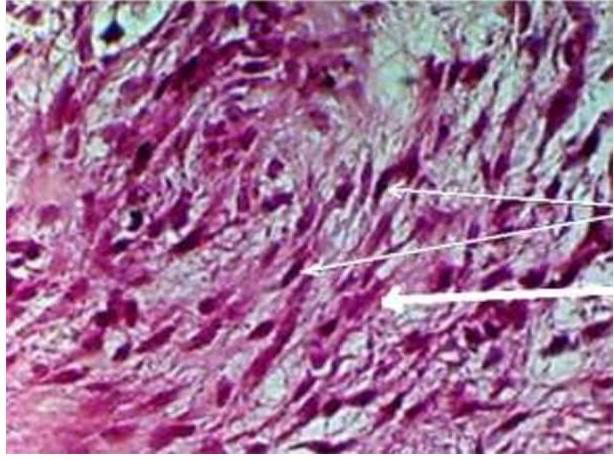
Figure 2: Cell block from a case of juvenile fibroma showing fibroblasts (thin arrows) and thick homogenous collagen bundles (white arrow). (H&E, x400).

Figure 3: FNAC smear from a case of dermoid cyst showing benign squamous degenerated cells (thin black arrow) and keratinous material (double arrow) in a background of cellular debris (white arrow). (H&E, x400).
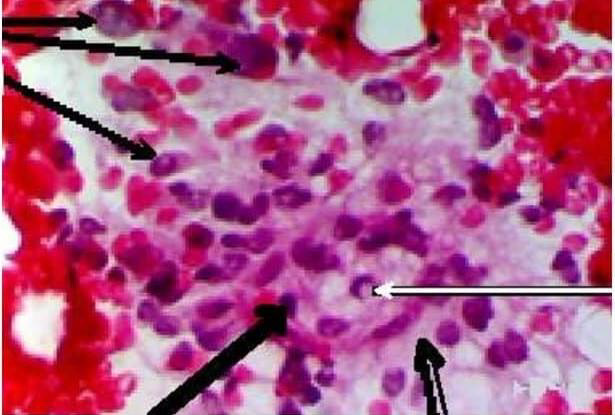
Figure 4: FNAC smear from case of atypical lipoma showing pleomorphic hyperchromtic cells (thin black arrows) and some with pseudo-inclusions in nuclei (thin white arrow). Some apoptotic bodies (thick black arrow) could be seen, but absent mitosis. The background is mucinous with slight vacuoles (double arrow). (H&E, x400).
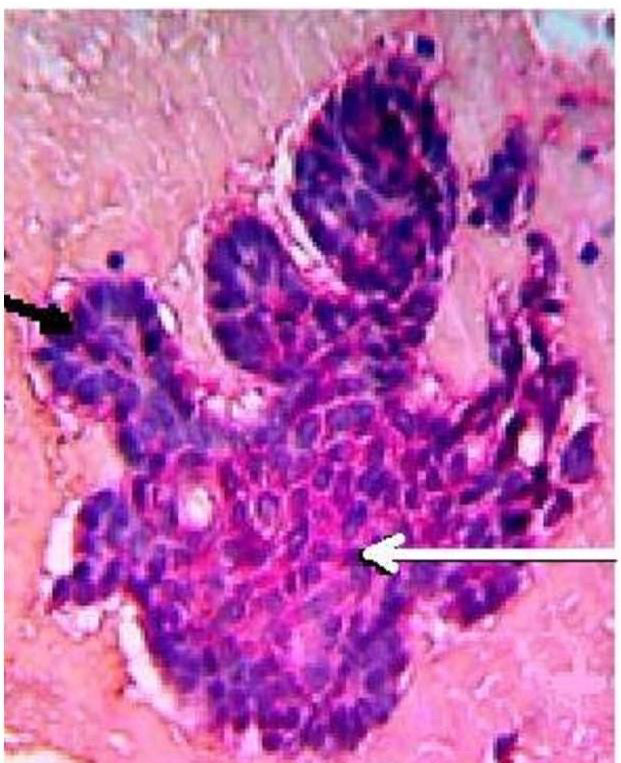
Figure 5: Cell block from a case of basal cell carcinoma, showing malignant basaloid cells (white arrow), peripheral palisading (black arrow). (H&E, x400).
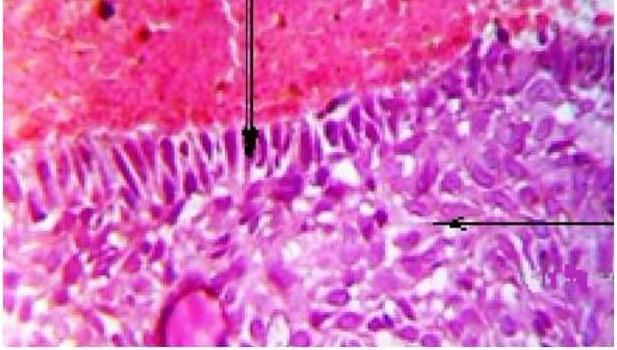
Figure 6: Cell block from a case of basal cell carcinoma showing malignant basaloid cells (double arrow) with peripheral palisading (arrow). (H& E, x400).
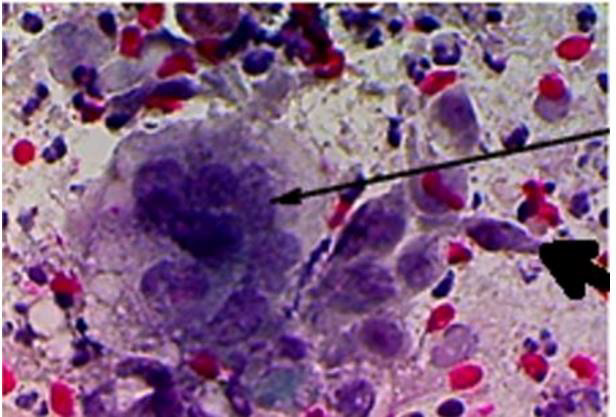
Figure 7: Cell block from a case of squamous cell carcinoma, showing; tap pole malignant squamous cell (thick arrow), overlapped malignant squamous cells (thin arrow). (PAP, x400).
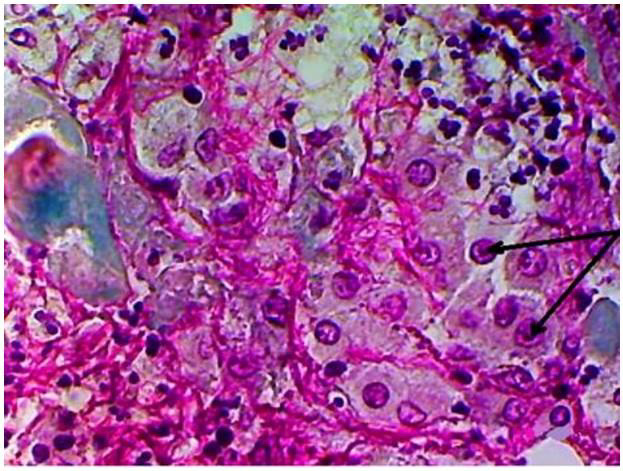
Figure 8: Cell block from a case of squamous cell carcinoma showing malignant squamous cells with prominent nucleoli (arrows). (PAP, x400).
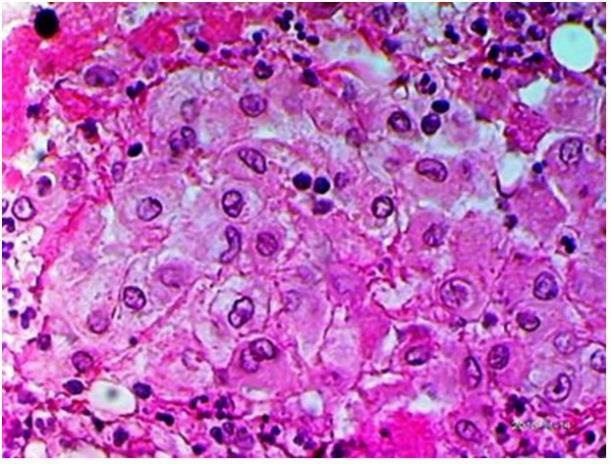
Figure 9: Cell block from a case of Squamous cell carcinoma showing pleomorphic malignant squamous cells. (H&E, x400).
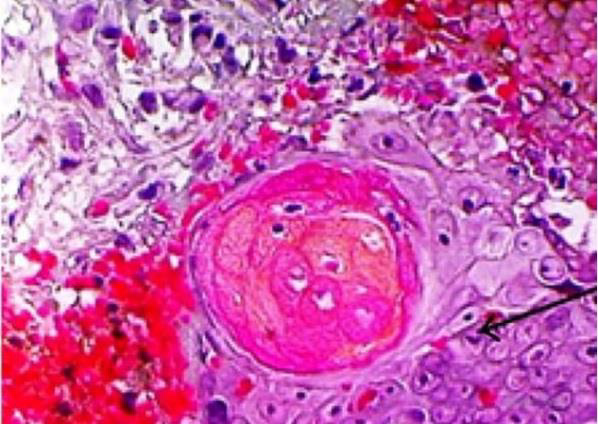
Figure 10: Cell block from a case of squamous cell carcinoma showing malignant squamous cells with prominent nucleoli (thin arrow), keratin pearls. (H& E, x400).
Discussion
In this study, we focused on the performance of cell mass and its importance in diagnosing and differentiating lesions due to its simplicity and reproducibility. We performed FNAC smear first, as it is a rapid test to detect the presence and types of cells in general and also to compare the features found in FNAC smear and those in cell blocks. FNAC is an easy to perform and inexpensive technique. It does not disturb the architecture of the lesion and has nothing to do with the promotion of metastasis of malignant lesions, because it is a non-invasive technique and does not harm the patient. It looks similar to intramuscular or subcutaneous injection of any medication using a fine needle. We utilized the clot method for preparation of cell blocks, other methods described by [9] and [10]. We preferred the clotting method because the structural forms of cells and tissues were more preserved. We utilized the same clotting method in preparation of cell blocks in two previous studies and gave excellent results [11]. Patients in this work ranged in age from 2 to 76 years with a greater transition to senescence (>40 years was about 70%), and the female to male ratio was 3 to 2, respectively with no significant outcome. This means that the appearance or complaint of the skin or subcutaneous nodules occurs more often in females and at older ages. For FNAC smear results, the test processed a sensitivity about 83% that is a significant percentage but lower than that of cell block (97.77%) This meant that cell block is more sensitive test than FNAC smear. Furthermore, cell block technique is more specific than FNAC smear, (100%) for cell block, and 16.66% for FNAC smear).
These results alluded to the role of cell block in appearance of cell orientations which give a picture resembling the tissue biopsy. Similarly, another study reported high sensitivity and specificity of FNAC in diagnosing skin lesions with sensitivity of up to 100% in epidermal cyst and inflammatory lesions, but showed only 67% for adnexal tumors [12]. The authors also reported specificity of 50% for adnexal tumors.In case of benign cyst, the cyst was filled of fluid, so the smear contains scanty cells, which may not appear, and the smear gave an insufficient result. Cell block provided more accurate result, but the performance of cell block may fail because of low cells and need gentle handling. In case of seborrehic keratosis, the smear was insignificant, because the cells were degenerated, with more brown pigmented cells; the features of cells were vague. On contrast in cell block, the benign features of cells were more obvious. This picture gives a confidence in diagnosis as a benign lesion. In cases of lipoma and fibrolipoma, the smear showed fat globules and/or mature fat cells, fibrous elements a picture found by other authors [13]. These features give a confidence of benign lesion, but the specific diagnosis cannot be achieved. The specific diagnosis of lipoma, fibrolipoma can be given easily in cell block. In cases of fibroma; the smear gave a suggestion of benign fibrotic lesion (spindle-shaped fibroblasts and some collagen fibers), but the cell block showed well-formed fibroma. In cases of juvenile fibromas, the smear may be negative because of the dense contents; however, the cell block is specific for diagnosis, moreover, it takes another importance to exclude juvenile fibrosarcoma and fibromatosis (the absence of mitotic activity).
On contrary of the previous lesions, FNAC smear provided satisfactory results that distinguished a benign lesion, and also specific for neurofibroma; because it gave us a picture of twisted nuclei, angulated and a hair-like background of neurofilaments a feature also found by [14]. In cases of pilomatrexioma, the smear gave a picture of benign lesion (ghost cells, mature epithelial cells, giant cells) the same picture found by[15], but the cell block failed in most cases because of the presence of admixed amounts of degenerated, or shadow cells. In cases of dermoid cysts or implantation cysts, the smear showed a mixture degenerated epithelial cells and keratinous material, a picture found also by [16], but the cell block also usually failed due to the keratinous material.In cases of atypical lipomas, FNAC smear showed a very useful picture; pleomorphic, hyperchromatic lipoblasts, mucoid background; the cell block did not add a more information. In cases of basal cell carcinoma; FNAC smear showed malignant cells with basophilic cytoplasm; the same results were found by [17], but the orientation of cells appeared in the cell block with peripheral palisading. In cases of squamous cell carcinoma, the malignant epithelial cells and the individual cell keratinization appeared in the smear. The FNAC smear showed a good picture but the specific feature of cell nests and keratin pearls appeared in the cell block. In cases of FNAC smear of basosqaumous cell carcinoma; the smear gave a picture of malignant epithelial cells, but the specific orientation of basosqaumous cell carcinoma appeared in the cell block,In cases of Madura foot, the smear showed mixed inflammatory cell infiltrate which was non-specific, but cell block was very useful to clarify the mycetoma colonies with appearance of peripheral esinophilic clubs; however, [18] could found this feature in the FNAC smear. The flowchart followed in the study and the main results are shown in Figure 11.
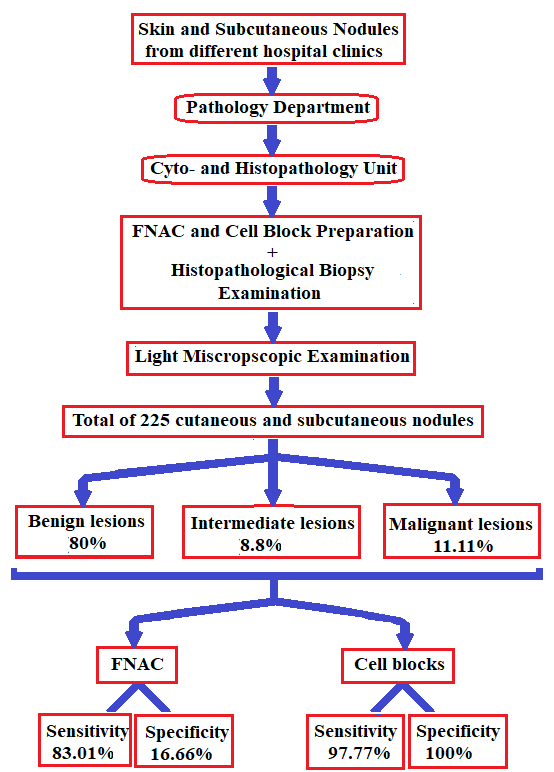
Figure 11: Flowchart showing main steps followed in the study and main findings.
Conclusion
Cell block study gives a more specific and more orientation
of the cells similar to that of tissue biopsy. FNAC smear may give
a useful advantage. Some lesions give negative results in smears,
others give negative results in cell block. Therefore, we recommend
performing FNAC smear as well as cell blocks whenever possible.
For more Articles on : https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.