Developmental Difficulties Prevalence and Management Capacities Among Children Including Genetic Disease in a Coastal District of India
Introduction
Birth defects (BD’s) are one of the most frequent conditions
that pediatricians experience in clinical practice. The major clinical
conditions can be grouped as genetic disorders and congenital
anomalies [1]. When the child fails to meet developmental
milestones related to daily living, it is considered as developmental
delay (DD) [2]. Over the past 12 years, the occurrence of DD’s
has increased by three percent in children under the age group
of five and has reached up to 15 % [3]. Worldwide, 1.5% -19.8%
of children have DD. In India, the children who are discharged
from the sick newborn unit have a high prevalence of DD’s. The
government of India initiated the 4D’s approach through District
early intervention center (DEIC) for the treatment and support of
these challenged children [4]. For ensuring proper health care for
children, it is necessary for early detection and in time management
of disorders [5]. If the DD’s are not intervened in time, it can lead
to manifested functional disabilities in children. In such cases, the
children are being subjected to treatment after the identification of
these disabilities [6].
DEIC is engaged with a team consisting of medical officers,
Pediatrician, Paramedics, and staff nurses and also provides
referral support to children (1month-18 years) diagnosed with
health conditions during the screening period. The present study
investigates the prevalence of the conditions screened among the
children attending the DEIC center at Visakhapatnam for the period
of 5 years (January-2016 to December-2020) and also to find out
the adequacy of institutional capacities in child health screening.
Materials and Methods
The present study was aimed to assess the burden of DD’s and
their trend in the DEIC, Visakhapatnam, and also to analyze the
availability of manpower as well as infrastructure, so as to suggest
possible improvements in the management of such diseases.
Necessary permission was obtained from the institutional ethics
committee, Andhra University, and also from the Andhra Medical
College in this regard. In this center, BD’s were diagnosed by the
pediatrician through a medical examination. As part of the study,
the registers of the patients admitted at the health center with DD’s
during 2016-2020 were reviewed on the lines of patient sex, age
and health condition including genetic disorder. Assessment of the
institutional capacities in child health screening was done taking
into cognizance of the Rashtriya bal swasthya karyakram (RBSK)
norms which were initiated by the government of India. During
and after the survey privacy and confidentiality were ensured. SPSS
Software Version 19 was used for data entry and analysis (SPSS
South Asia Pvt. Ltd, Banglore, Karnataka).
Quantitative and Qualitative research methodologies were
utilized to evaluate the administration rehearses on (developmental
delays) DD’s at the chosen health facilities. The study instruments
were office agenda; record survey for specific administrations over
the most recent one year; and semi-organized schedule of interview
for administration providers. Security and privacy were kept up
during and after the review. Information passage and investigation
were done in SPSS Software Version 19 (SPSS South Asia Pvt. Ltd,
Banglore, Karnataka).
Results
Total 26423 children with DD’s consulted the DEIC during the investigation time frame. These children were classified under the 4D’s (i.e., defects, deficiencies, diseases, and disabilities) approach. From the results tabulated in Graph 1, it can be observed that children below 6 weeks age group are 4786 (18.11%) numbers, of which 2508 are male and 2206 are female. The age group of one and a half month old to 3 years old, total 6397 (24.20%) kids was there of which 3619 are male and 2778 are female; and in 3 years to 6 years category, 3325 are male and 2006 are female totaling to 5331 (20.17%) numbers. Children between 6 years to 18 years old are 9909 (37.50%) numbers involving 5408 males and 4501 females. The children having conditions under each of the 4D’s are tabulated under the graph 2, 3, 4, and 5 respectively.
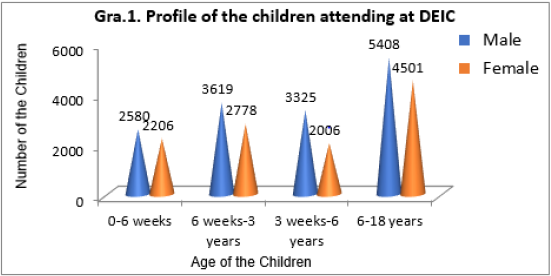
Graph 1: Profile of the children attending at DEIC.
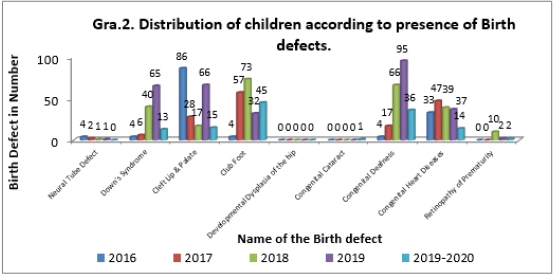
Graph 2: Distribution of children according to presence of birth defects.
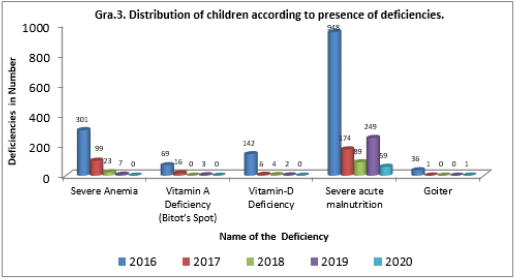
Graph 3: Distribution of children according to presence of deficiencies.
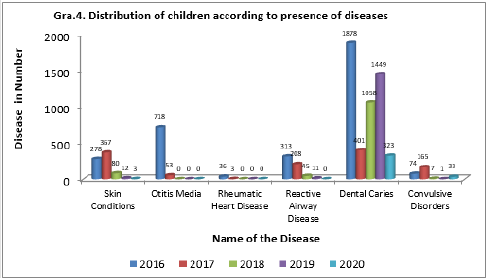
Graph 4: Distribution of children according to presence of diseases.
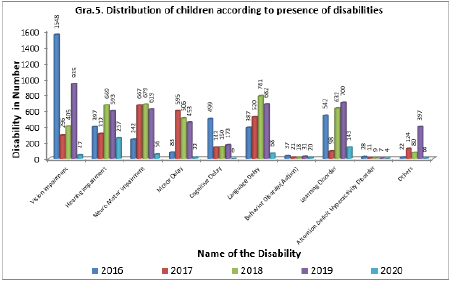
Graph 5: Distribution of children according to presence of disabilities.
Graph 2 shows the distribution of children according to the presence of BD’s for the last five years. The different birth defects screened by the center are neural tube defect, down’s syndrome, cleft lip & palate, club foot, developmental dysplasia of the hip, congenital cataract, congenital deafness, congenital heart diseases, and retinopathy of prematurity. Out of 135 BD’s cases identified in 2016, the majority of cases were cleft lip & palate cases with 86 (63.70%) numbers followed by congenital heart disease cases with 33 (24.44 %) numbers. In 2017, the total BD’s are 157 out of which club foot cases were maximum with 57 (36.30 %) numbers and congenital heart diseases cases come next with 47 (29.93%) numbers. In 2018 total number of these cases are 246, of which club foot cases were maximum with 73 (29.67%) numbers followed by congenital deafness cases with 66 (26.82%) numbers. During the year 2019, a total of 298 cases was identified with congenital deafness in a maximum of 95 (31.87 %) numbers followed by cleft lip & palate cases in 66 (22.14 %) numbers. For the year 2020, a total of 126 cases was found, comprising the highest number of club foot cases in 45 (35.71%) children and congenital deafness cases in 36 (28.57%) children. From all the above it is observed that the highest number of BD’s occurred in 2019 and dropped to their lowest among children in 2020. However, while studying the trends in BD’s data for a selected five-year period, it was observed that the prevalence rate of cleft lip & palate, club foot, and congenital deafness cases is much higher.
Graph 3 shows the distribution of children according to the presence of deficiencies. These are severe anemia, vitamin A deficiency (bigot’s spot), vitamin-D deficiency, severe acute malnutrition, and goiter. The number of deficiencies is 1496, 296, 116, 261, and 60 for the years 2016, 2017, 2018, 2019, and 2020, respectively from the center. The deficiencies have diminished from a maximum of 1496 cases during the year 2016 to a minimum of 60 cases in the year 2020. During the total period of the study, it is observed that most of the children are suffering from severe acute malnutrition followed by severe anemia. To overcome this problem, a nutritional rehabilitation center was attached to this institute and is located in King George hospital, Visakhapatnam. With the help of this rehabilitation center, the nutritional status of the needy children is being improved.
Graph 4 indicates the distribution of children according to the presence of diseases. Among the list of diseases, skin conditions, otitis media, rheumatic heart disease, reactive airway disease, dental caries, and convulsive disorders were present. The number of diseases is 3297, 1197, 1190, 1473, and 359 from the center for the years 2016, 2017, 2018, 2019, and 2020, respectively. During the total period of the study dental caries were found in a maximum number of children and the second most common disease found was otitis media. Year by year there is a gradual decline in the number of cases with diseases and this is due to public awareness and stringent steps taken by the government towards diseases.
Graph 5 demonstrates the distribution of children according to the presence of disabilities. Among these vision impairment, hearing impairment, neuromotor impairment, motor delay, cognitive delay, language delay, behavior disorder (autism), learning disorder, attention deficit hyperactivity disorder, and other inabilities like growing up concerns, substance abuse, feel depression, delay in period cycles, torment during the period, agony or copying sensation while peeing and release/Foul-smelling release from the genitourinary zone. 3785 disability cases were found in 2015- 2016, of which there were a maximum of 1548 (40.89%) vision impairment cases followed by common learning disorder cases with 542 (14.31%) numbers. In 2017 the total cases coming under disability are 2787 of which neuromotor impairment cases were the highest with 667 (23.93%) numbers and motor Delay cases were the next with 595 (21.34%) numbers. In 2018 the total cases under this section are 3929, in which language delay cases are topping the list with 781 (19.87 %) numbers followed by neuromotor impairment cases with 667 (16.97%) numbers. During the years 2019 and 2020 the total number of cases under this category are 4590 and 625 respectively of which vision impairment, hearing impairment, and learning disorders have mostly occurred. While studying the data, it is observed from the trends in disabilities for the selected period that the occurrence rate of vision impairment and language delay disorders was much higher.
On investigation of the institutional amenities like manpower and diagnostic services accessible in the DEIC, it is observed that the posts of a pediatrician, dental specialist, physiotherapist, optometrist, audiologist cum speech therapist, early interventionist cum exceptional instructor, lab technician, staff nurse-1, staff nurse-2, and social worker were filled as per the sanctioned strength and they were working throughout the study period. The post of a medical officer, psychologist, and manager stayed empty all through the examination time frame. Pediatricians and 40 % of supporting staff are having knowledge of genetic testing and awareness towards genetic disease management. Regular record maintenance is taking place in this center; however, much information related to genetic disorders is missing. Also observed that the center does not have genetic counselors. It was found that there are no investigation facilities for genetic diseases. Related diagnostic tests were virtually non-existent in the center with the exception of basic blood, serum, and urine diagnostic tests. The needy children are being referred to KGH or private diagnostic laboratories for specific genetic tests and for confirmation.
Discussion
BD’s are persisting throughout the world. Due to the high
mortality rate of affected infants in low-income countries, it can
be admitted that the impact of birth defects is higher in these
countries. Even in the children who have BD’s and still survive, due
to no timely intervention, these disorders are causing irreversible
lifetime complications with mental or physical disabilities and
these children are about 3.2 million in number around the world
per each year [7]. The present study found a significantly increased
prevalence of BD’s in children in the selected region. Our study
revealed that a total of 26,423 cases were admitted through the 5
years period. This prevalence is higher than that reported by prajna
Bhide and Anita Kar wherein it was stated that the affected births
with surveillance of congenital anomalies are as many as 472,177
in India each year [8].
The findings of the present study reveal that the gender
distribution of admitted patients is 14932 (56.51%) male and
11491 (43.48%) female. Such a study is also made in the past by
Valla et al and it was identified that the male sex is associated with
a high risk of having DD’s [9]. Another previous study by Dabar et
al. illustrates that there is no relationship between gender and DD’s
[10]. With regard to BD’s, our findings provide evidence of the rise of
these defects over time. Majority children had congenital deafness
(218; 22.66%) followed by cleft lip & palate (212, 22.03%). Our
study confirms the findings of several other studies which reported
that the prevalence of congenital deafness is more in India and 63
million people suffer from significant auditory loss, due to a lack
of skilled manpower and human resources for the management of
these defects [11]. The second most common defect was cleft lip
& palate. Our estimates however have to be considered as bestavailable
data, as previous analysis on the cleft lip in south India
also reported similar findings [12,13].
In respect of deficiencies, during the selected study period the
most common deficiency was severe acute malnutrition with 1519
(68.14%) cases followed by severe anemia with 430 (19.29%) cases.
Our findings are also supported by one of the previous surveys
conducted by measuring weight for height during a ten-year period
which states that children under the age of five years are mostly
suffering from severe acute malnutrition [14]. Regarding anemia,
similar findings reported by Avina Sarna et al., who identified that
the prevalence of anemia is higher from newborns to adolescents
in India [15].
Regarding diseases, it is observed that most of the children had
dental caries. The admission trend of these cases is high in 2016
and then declined in the next year and again rises from 2017 to
2019. Previous findings by Abhishek Mehta et al., are supporting
these trends, wherein it was reported that a large number of Indian
children have been affected by dental caries [16]. In the present
study, we also observed a gradual declining trend of otitis media,
skin conditions, and reactive airway disease. Similar findings were
observed in the previous studies that the prevalence of otitis media
[17], skin conditions [18], and reactive airway disease [19] are low
during the past years. This is probably due to the reason that the
people are now much aware of these diseases, and they approach
the health care personnel in time.
From the side of disabilities, vision impairment has occurred
in most of the children in about 3231 (20.55%) numbers and the
occurrence was alternatively rising and declining through the years.
Similar findings were observed by Murthy et al., that the incidence
and prevalence of loss of sight in children is varying during their
study period in India [20]. This was followed by language delay
with (2438, 15.51%) cases, and their occurrence has risen from
2016 to 2018 and then declined. Overall, these results are slightly
higher when compared to the prevalence in developed countries as
reported by Wren [21]. The present study reveals that the trend of
admission of neuromotor impairment cases was being consistent
with a large number up to 2019 and then diminished. In the past,
population-based studies reported that the neurological disorders
in rural India are higher and were found in about 6-8 million people
[22]. The present study divulges that the peak incidence of deafness
was during 2018; and this finding corroborates with the study
findings of Nagapoornima et al. wherein it was reported that due
to failure of timely screening of newborns, most of them are facing
hearing impairment in India [23].
Institutional facilities are labor and infrastructural facilities and
are important in offering quality assistance to children regarding
genetic disease management. In the present study, on examining
the manpower we observed that the medical officer, psychologist,
and manager were not available throughout the study period. Due
to the non-availability of manpower in such key posts, there is a
devastating effect on the treatment of the kids with DD’s. The rest of
the working staff from DEIC, Visakhapatnam are well aware of their
respective duties in the management of these disorders. Further,
only basic biochemical tests are being conducted in the center and
there are no specific genetic testing facilities available here. Private
diagnostic laboratories in the city are being referred to for genetic
tests. With regard to public health concerns, Institutional facilities
form the foundation for improving public health. The entire public health services are dependent on the availability of basic
infrastructural facilities and manpower capacities [24].
Conclusion
Through this study, the institutional facilities at DEIC, Visakhapatnam as well as the high incidence of birth defects in Visakhapatnam district were observed. The study discloses the need for strengthening management services for these disorders in this region so that the prevalence of birth defects can be minimized. National health agencies use such data for the design and evaluation of birth defects. The proposals for better management of birth defects in the selected area are; increasing the number of genetic testing units, improving the skills and expertise of the health care personnel with respect to birth defects, and developing national policies for reinforcing related services. In addition, more extensive studies are needed across the nation to determine the distribution of birth defects and their causes for overall understanding and management of the same.
For more
Articles on : https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.