Lession Inconsistent with Serum β-hCG for Intramural Pregnancy Monitoring
Introduction
Intramural pregnancy (IMP) is a rare type of ectopic pregnancy and described as a pregnancy that is partially or completely located within the myometrium of the uterine wall without communication with the endometrial cavity [1]. The cause of IMP remains unclear, endometrial, and uterine serosa damage or defect [2], adenomyosis and in vitro fertilization [3] are considered to increase the risk of IMP. The clinical symptoms are a history of amenorrhea with high serum β-human chorionic gonadotropin (HCG) levels, abdominal pain, irregular bleeding of the vagina, even the rupture of the uterus led to hemorrhagic shock [2-3]. However, the clinic typical are non-specificity in the early, similar to early pregnancy, other types of ectopic pregnancy and gestational trophoblastic neoplasia (GTN), resulting in difficult to diagnose. Serum β-hCG and imaging, transvaginal ultrasound (TVS) and magnetic resonance (MR) imaging, have been used for diagnosis of IMP recent years, however, their role in monitoring IMP has not been elaborated. Herein, we report a patient whose serum β-hCG level had a steady decline later without intervention, however, the lesion in TVS keep growing.
Case Report/Presentation
A 34-year-old female patient (G5P2), who had a history of induced abortion 14 days ago, was with prolonged vaginal bleeding underwent TVS and pregnancy test, and the result showed that a 12mm lesion was within the myometrium (Figure 1(A1)), and the serum β-hCG was positive (5203 mIU/ml) (Figure 1E). And then her serum β-hCG level had a steady decline later without intervention (Figure 1E), however, the lesion keeps growing (Figures 1(A1-D1) & 1F) with the enhancement of color Doppler signals (Figures 1(A2-D2)). One week later, her serum β-hCG level was 3299 mIU/ mL (Figure 1E) while the lesion embedded into the myometrium in the right-side wall of the uterine increased to 24 mm (Figure 1(B1)). Then a 40mm diameter mass was detected by TVS after 28 days (Figures 2A & 2B), and 3-D MR reconstructions confirmed the diagnosis of intramural pregnancy (Figure 2C). Thereafter, the patient was admitted to hospital, local mass resection by laparoscopy was performed. Intraoperative freezing showed spindle cell tumor, and postoperative histopathology confirmed it. Her β-hCG decreased to 50.4 mIU/mL 10 days after surgery with no vaginal bleeding and returned to normal 2 months after surgery (Figure 1G).
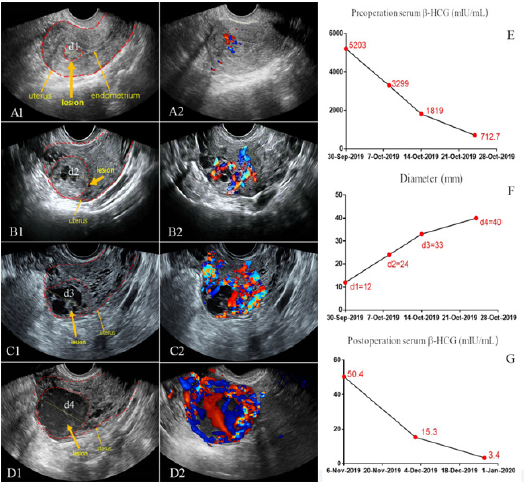
Figure 1: Image and serum β-hCG change for suspected intramural pregnancy monitoring
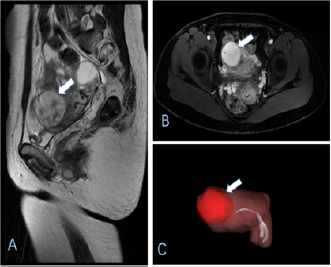
Figure 2: MR image and 3-D MR reconstructions for 40mm diameter mass in uterine.
Discussion/Conclusion
IMP accounting for less than 1% of all ectopic pregnancies [4], which is increased significantly in recent years. The main symptoms of IMP are menopause, mild vaginal bleeding, abdominal pain and increasing of serum β-hCG [5], however, they are seldom specific in early, which make IMP is too difficult to diagnose. Numerous patients are not diagnosed IMP until uterine rupture [6]. Thus, early diagnosis and monitoring are the key to prevent complications. Nowadays, TVS is considered as the first-line imaging technique for diagnosis of ectopic pregnancy, however, the data to monitor intramural pregnancy is absent [7]. MR imaging has been reported be useful in the early diagnosis of IMP [8] by providing a clear definition of the relationship between the identified lesion and the endometrial cavity, however, imaging features are very similar to GTN, resulting in especially challenging in diagnosis. The treatment for patients with IMP should be individualized, depending on the size of the lesion, patient status and the desire for future fertility. At present, the major treatment is surgery and medical therapy. Firstly, surgery for IMP include mass resection by laparoscopy or hysterectomy by laparoscopy or open surgery [4]. In our case, we found a lesion was within the myometrium 14 days after induced abortion. Besides, the diameter of lesion increased with time, thus mass resection by laparoscopy was performed. Secondly, verghese, et al. [9] reported the successful management of IMP with systemic methotrexate administration. A number of patients reached clinically cured by methotrexate.
Besides, a few treatments using UAE in the literature also has been reported [10]. LONG, et al. reported the successful management of an intramural pregnancy in the second trimester with individualized and combined [11]. In summary, our observation nicely illustrates serum β-hCG level should combined with image for suspected intramural pregnancy monitoring. Early diagnosis of intramural pregnancy is often difficult, and image change may help to make an accurate diagnosis.
| For more Articles on : https://biomedres01.blogspot.com/ |




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.