Pneumothorax Associated with Thoracic Endometriosis: Current Knowledge
Introduction
Endometriosis is a condition in which endometrial-like glands and stroma are located outside of the uterine cavity. The ectopic endometrium is encountered most commonly pelvic structures such as ovary, uterine ligaments, pelvic peritoneum, and genital structures [1-4]. The usual site of endometriosis outside of the abdominopelvic cavity is in or around the lung (intrathoracic cavity) (Figure 1). Although endometriosis in general can affect up to 15% of women of reproductive age, thoracic endometriosis remains a very rare condition [5-9]. Thoracic endometriosis produces a broad range of clinical and radiological manifestations, including catamenial pneumothorax (80%), catamenial hemothorax (15%), hemoptysis (5%), and rarely pulmonary nodules [5-9]. The age of onset in patients with thoracic endometriosis (a mean of 35 years) is higher compared to a mean age at presentation of 25 to 30 years in patients with only pelvic endometriosis [5-9]. The exact mechanism of catamenial pneumothorax associated with thoracic endometriosis remains unclear, but several hypotheses have developed to explain this condition.
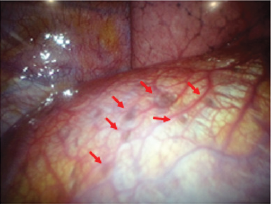
Figure 1: Endometriosis involving the pleural surface of diaphragm (arrows). The clinical and laboratory findings have been reported previously [32].
Retrograde Menstruation through Diaphragmatic Fenestrations
The endometrial tissue is thought to move through the fallopian tubes to the peritoneal cavity by retrograde menstruation backflow [4]. The endometrial cells in peritoneal fluid may follow clockwise peritoneal circulation and pass through the right paracolic gutter towards the right sub-diaphragmatic region. The phrenicocolic ligament on the left side and falciform ligament form barriers that prevent cells and fluids from reaching the left sub-diaphragmatic area [10,11]. Implantation of endometrial cell leads to the formation of endometriotic nodules on the ventral side of the diaphragm [10]. The nodules cause cyclical necrosis and induce diaphragmatic fragility, leading to the formation of the usual diaphragmatic fenestrations. After endometrial tissue enters the pleural space, it may form colonies in other part of the diaphragm or in the pleural space. Air leaks from vagina may occur during the menstrual cycle when the cervical mucus plug is deleted [10-14]. This hypothesis may be in good agreement with the observation that endometriosis occurs nine times frequently on the right hemidiaphragm than on the left [4,6,14,15].
Coelomic Metaplasia
The second proposes the coelomic metaplasia mechanism that causes endometriosis by metaplasia of mesothelial cells lining the pleura and peritoneal surfaces into endometrial stroma and gland [9,16,17]. Transformation of these cells may be affected by physiological stimuli such as estrogen [18]. Support for this hypothesis is observed in endometriosis patients with Mayer- Rokitansky-Küster-Hauser syndrome who lack a functional endometrium [19,20]. Rare cases of endometriosis can also occur in men receiving high-dose estrogen. The coelomic metaplasia hypothesis provides an explanation for pleural cases of thoracic endometriosis. However, this fails to explain the right-sided predominance seen in patients with thoracic endometriosis.
Prostaglandin
The third is a bioactive substance-mediated mechanism in which high levels of prostaglandins, in particular prostaglandin F2α. Prostaglandins are detectable in the plasma of women during menstruation. Circulating prostaglandins increase with menstruation [21,22-25] and causes vascular and bronchiolar vasoconstriction, leading to the vasospasm and associated ischemia within the lung [23,25,26]. This may result in alveolar rupture of previously formed subpleural blebs and bullae, and subsequent air leaks [23,25-27].
Hematogenous or Lymphatic Metastasis
An interesting hypothesis of metastasis suggests that endometrial transplantation occurs through lymphatic or hematogenous dissemination of endometrial cells, explaining both the thoracic and other sites of implantation, in an analogous manner to cancer metastasis [7,28,29]. Review of autopsy data of humans with thoracic endometriosis shows that patients with bronchopulmonary endometriosis usually have bilateral lesions, whereas diaphragmatic and pleural diseases are predominantly right sides [17]. Perhaps the most compelling evidence for the benign metastasis hypothesis is derived from the investigations of ectopic endometriosis lesions occurring in remote parts of the body including the bone or brain [8,21,30-32].
Comment
Thoracic endometriosis is characterized by the presence of endometrial-like glands and stroma within the lung parenchyma or on the diaphragm and pleural surfaces. It remains unclear how endometrial tissue migrates to the thoracic cavity, but it is often associated with abdominal endometriosis. As none of the theories proposed alone can account for all clinical manifestations of this condition, so the etiology of thoracic endometriosis development is likely multifactorial and closely intertwined with each other hypothesis.

No comments:
Post a Comment
Note: Only a member of this blog may post a comment.