Influence of Abrasive Peeling of Wheat-Tritical Grinding Grain Mixture on the Yield of Intermediate Grinding Products and Flour
Introduction
Current directions of development of one of the most important branches of the processing industry - flour milling is both the improvement of technologies for processing traditional crops (wheat and rye), and the development of new technologies for processing non-traditional crops, such as triticale [1-2]. One of the main directions of development of the industry is the development of new and improvement of traditional technologies and the creation of processed products of various types of grain with a given composition and properties, including products of deep processing [3-5,6,7]. In addition, the direction of joint processing of grain of various crops, including wheat and triticale, is very promising. Triticale is the first grain crop created by man and obtained by crossing wheat (Latin Triticum) and rye (Latin Secale). The use of triticale as a food crop is an interesting, promising direction not only for the flour milling, but also for other branches of the food and processing industries. This is confirmed by the increased interest in this culture, both from researchers and from food producers not only in our country, but also abroad. Bakery products using processed products from the central part of the endosperm of triticale grain are characterized by increased nutrition due to a higher protein content and essential amino acids, in particular the main limiting acid - lysine [8-11]. The combination of positive properties of rye - a high content of biologically active aromatic substances and wheat - the rheological properties of the dough, allow making food products of mass consumption from processed products of triticale grain and mixtures based on it.
At the same time, the technological properties of baking flour obtained from various grain mixtures, including wheat-triticale grain grinding mixture, remain poorly understood. Peeling of the wheat-triticale grain mixture during varietal bakery grinding is carried out for maximum cleaning of the grain surface from dust, dirt, mold, bacteria, as well as reducing and simplifying the length of the technological scheme [12-14]. Removal of surface shells with the use of peeling machines allows, in addition, to reduce the number of peeling and grinding systems and reduce the technological process of processing the milling wheat-triticale grain mixture into flour.
When using abrasive peeling in the finished product, the number of shell particles is reduced, and its appearance is improved [15,16]. The ash content of the milling grain mixture of wheat and triticale decreases after peeling. Removal of membranes allows: - get a more solid and hygienic clean product; - to obtain from the stripped systems bakery flour with a higher index of whiteness; - significantly reduce the number of grinding and sieve systems, simplify the technological scheme of grinding. In addition, it should be noted that in the process of peeling from the surface of the grain, not only impurities are removed, but also part of the fruit and seed shells. This, on the one hand, has a positive effect on reducing the process of moistening the grain, but on the other, due to the exposure of the endosperm and injury to the germ of the grain, it can lead to a loss of its viability, which is not given enough attention.
In this regard, additional studies of the peeling process and its effect on the properties of wheat grain are required [14]. The purpose of our research is to determine the effect of abrasive peeling on the yield of intermediate products of grinding and flour in the processing of peeled wheat-tritical grain mixture in varietal bakery grinding.
Research Materials and Methods
In studies conducted at the Department of Grains, Bakery and Confectionery Technologies of the Federal State Budgetary Educational Institution of Higher Education “MSUPP” and at the Department of Food Technologies and Organization of Restaurant Business at the I.S. Turgenev Oryol State University, experiments were conducted to determine the effect of the degree of peeling of the wheat-triticale grain mixture on the output of intermediate grinding products. The objects of research were wheat of the “Radmira” variety and triticale of the “Nemchinovsky 56” variety, bred by breeders of the Federal Research Center “Nemchinovka” and differing from other wheat varieties by the increased protein content of the 2020 harvest. The main physical, chemical and chemical parameters of the initial wheat-triticale grain mixture are as follows: humidity - 11.2%, ash content - 1.83%, protein content - 13.2%, gluten content - 23.8%, gluten quality - 79 units of the device, vitreousness - 46% and drop rate - 354 seconds. When preparing the wheat-tritical grain mixture for laboratory grinding as a hydrothermal treatment (GTO), a mandatory operation for varietal grinding, cold conditioning was used as the most common method and the cheapest method. After hydrothermal treatment, abrasive peeling was carried out before grinding wheat-tritical grain mixtures. For grinding, a laboratory grinding mill MLP-4 with rifled rollers with a groove arrangement of the back along the back was used.
The main mechanical and kinematic indicators of the mill MLP- 4 with rifled rollers are as follows: productivity - up to 100 kg / h, the speed of the fast-rotating roller is 4.5 m / s, the differential is 1.75, the location of the backrest grooves, the number of grooves on the 1st linear centimeter - 8 pieces, the slope of the grooves is 8%.
The intervalian clearance on the I drain system was 700 μm, on the II drana system - 300 μm, on the III drana system - 150 μm and on the IV dranaya system - 100 μm. When conducting studies to determine the effect of the number of removed shells in abrasive peeling of wheat-triticale grain mixtures on the yield of intermediate products of grinding, laboratory grindings of shelled wheat-triticale grain mixtures were carried out with preliminary removal of shells in the amount of 2.5%, 5.0%, 7.5%, 10% and a control sample without peeling.
Next, laboratory grindings were carried out and 4 of the 5 main, cereal-forming dredge systems were modeled when grinding the initial wheat-triticale mixture and peeled wheat-triticale grain mixtures. The data obtained to determine the effect of abrasive peeling on the grain-forming ability of peeled wheat-triticale grain mixtures are presented in (Tables 1-5).
As can be seen from (Table 1), the yield of intermediate grinding products during the processing of the initial wheat-triticale grain mixture without peeling, sent for grinding to grinding systems, was 63.6%, the yield of wheat-triticale flour was 12.0%, the yield of a similar product sent to the V draught system was 19.3%. As can be seen from Table 2, the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 2.5%, sent for grinding to grinding systems was 67.4%, the yield of wheat-triticale flour was 12.1%, the yield of a similar product sent to the V strip system was 17.8%.As can be seen from (Table 3), the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 5.0%, sent for grinding to grinding systems was 65.3%, the yield of wheat-triticale flour was 12.5%, the yield of a similar product sent to the V strip system was 17.1%. As can be seen from (Table 4), the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 7.5%, sent for grinding to grinding systems was 67.6%, the yield of wheat-triticale flour was 13.3%, the yield of a similar product sent to the V draught system was 16.9%. As can be seen from (Table 5), the yield of intermediate grinding products during the processing of a peeled wheat-triticale grain mixture with a removal of 10.0%, sent for grinding to grinding systems was 68.7%, the yield of wheat-triticale flour was 14.1%, the yield of a similar product sent to the V strip system was 15.4%. Thus, according to the results of the studies, it was found that the greatest yield of intermediate products of grinding and flour during the processing of the wheattriticale grain mixture is obtained by removing 10% of the shells and is 82.8%, which is 6.9% more compared to the original nonpeeled grain.

Table 1: Yield of intermediate products of grinding and flour of the initial wheat-triticale grain mixture without peeling.
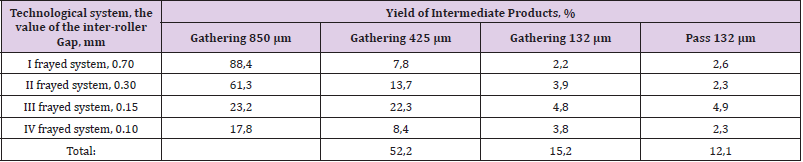
Table 2: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grainmixtures with the removal of 2.5% of the shells.
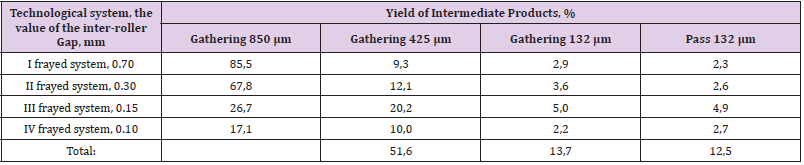
Table 3: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grain mixtures with the removal of 5.0% of the shells.
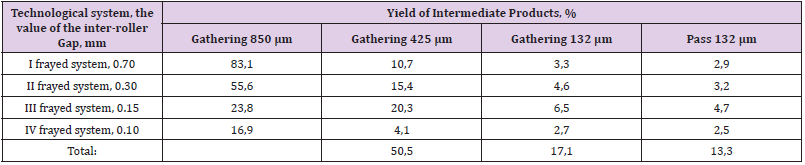
Table 4: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grain mixtures with the removal of 7.5% of the shells.
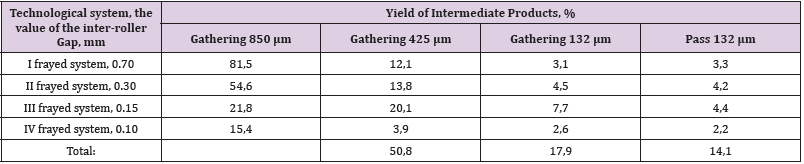
Table 5: The yield of intermediate products of grinding and flour during the processing of hulled wheat-triticale grain mixtures with 10% shell removal.
Findings
Thus, according to the results of the studies, it was found that abrasive peeling with the removal of up to 10% of the shells of wheat-tritical grain mixtures before grinding into varietal baking flour has a positive effect on the cereal-forming ability and leads to an increase in the yield of intermediate cereal grinding products and an increase in the yield of flour on the pulled systems. The greatest yield of intermediate products of grinding and flour during the processing of the initial wheat-tritical grain mixture is obtained by removing 10% of the shells and is 82.8%, which is 6.9% more compared to the original non-peeled wheat-tritical grain mixture.
For more Articles on: https://biomedres01.blogspot.com/