Comparison of Calcium, Chlorine, Iodine, Potassium, Magnesium, Manganese, and Sodium in Thyroid Tissue Adjacent to Thyroid Malignant and Benign Nodules
Introduction
Thyroid benign and malignant nodules (TBN and TMN, respectively) are the most common endocrine disorder worldwide. Moreover, in some parts of the world, especially those of current or former iodine deficiency, Thyroid Nodules (TN) are still an endemic disease [1]. Incidence of TBN and TMN has been growing steadily over the past four decades, despite the use of iodine prophylaxis in many countries [2]. Some factors causing this higher incidence of TN were described in literature [3] and analysis of these data shown intriguing links between the etiologies of TBN and TMN [2,3]. In other words, the factors contributing to increases in the incidence of TBN are the same as those contributing to increases in TMN. However, the current state of knowledge regarding TN demonstrates that the etiology and pathogenesis of TBN and TMN are still not enough understood, because there are many not adequately explored chemicals, which induced thyroid hormone perturbations leading to these diseases. For over 20th century, there was the dominant opinion that TN is the simple consequence of iodine deficiency [4].
However, it was found that TN is a frequent disease even in those countries and regions where the population is never exposed to iodine shortage. Moreover, it was shown that iodine excess has severe consequences on human health and associated with the presence of TN [5-8]. It was also demonstrated that besides the iodine deficiency and excess many other dietary, environmental, and occupational factors are associated with the TN incidence [3,9- 11]. Among these factors a disturbance of evolutionary stable input of many chemical elements (ChEs) in human body after industrial revolution plays a significant role in etiology of TN [12]. Besides iodine, many other ChEs have also essential physiological functions [13]. Essential or toxic (goitrogenic, mutagenic, carcinogenic) properties of ChEs depend on tissue-specific need or tolerance, respectively [13]. Excessive accumulation or an imbalance of the ChEs may disturb the cell functions and may result in cellular proliferation, degeneration, death, benign or malignant transformation [13-15]. In our previous studies the complex of in vivo and in vitro nuclear analytical and related methods was developed and used for the investigation of iodine and other ChEs contents in the normal and pathological thyroid [16-22]. Iodine level in the normal thyroid was investigated in relation to age, gender and some non-thyroidal diseases [23,24].
After that, variations of many ChEs content with age in the thyroid of males and females were studied and age- and genderdependence of some ChEs was observed [25-41]. Furthermore, a significant difference between some ChEs contents in colloid goiter, thyroiditis, thyroid adenoma and cancer in comparison with normal thyroid was demonstrated [42-47]. The present study was performed to clarify the role of some ChEs in the etiology of TBN and TMN. Having this in mind, the aim of this exploratory study was to examine differences in the content of Calcium (Ca), Chlorine (Cl), Iodine (I), Potassium (K), Magnesium (Mg), Manganese (Mn), and Sodium (Na) in thyroid tissue adjacent to TN using a nondestructive instrumental neutron activation analysis with high resolution spectrometry of short-lived radionuclides (INAA-SLR), and to compare the levels of these ChEs in two groups of samples (tissue adjacent to TBN and TMN, respectively). Moreover, for understanding a possible role of ChEs in etiology and pathogenesis of TN results of the study were compared with previously obtained data for the same ChEs in “normal” thyroid tissue [42-47].
Material and Methods
All patients suffered from TBN (n=79, mean age M±SD was 44±11 years, range 22-64) and from TMN (n=41, mean age M±SD was 46±15 years, range 16-75) were hospitalized in the Head and Neck Department of the Medical Radiological Research Centre (MRRC), Obninsk. Thick-needle puncture biopsy of suspicious nodules of the thyroid was performed for every patient, to permit morphological study of thyroid tissue at these sites and to estimate their trace element contents. In all cases the diagnosis has been confirmed by clinical and morphological results obtained during studies of biopsy and resected materials. Histological conclusions for benign nodules were: 46 colloid goiter, 19 thyroid adenoma, 8 Hashimoto’s thyroiditis, and 6 Riedel’s Struma, whereas for thyroid malignant tumors were: 25 papillary adenocarcinomas, 8 follicular adenocarcinomas, 7 solid carcinomas, and 1 reticulosarcoma. Samples of visually intact thyroid tissue adjacent to TBN and TMN were taken from resected materials.
“Normal” thyroids for the control group samples were removed at necropsy from 105 deceased (mean age 44±21 years, range 2-87), who had died suddenly. The majority of deaths were due to trauma. A histological examination in the control group was used to control the age norm conformity, as well as to confirm the absence of micro-nodules and latent cancer. All studies were approved by the Ethical Committees of MRRC. All the procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments, or with comparable ethical standards. Informed consent was obtained from all individual participants included in the study. All tissue samples obtained from tumors and visually intact tissue adjacent to tumors were divided into two portions using a titanium scalpel to prevent contamination by ChEs of stainless steel [48]. One was used for morphological study while the other was intended for ChEs analysis. After the samples intended for ChEs analysis were weighed, they were freeze-dried and homogenized [49]. The pounded samples weighing about 10 mg (for biopsy) and 100 mg (for resected materials) were used for ChEs measurement by INAA-SLR.
To determine contents of the ChE by comparison with a known standard, Biological Synthetic Standards (BSS) prepared from phenol-formaldehyde resins were used [50]. In addition to BSS, aliquots of commercial, chemically pure compounds were also used as standards. Ten sub-samples of Certified Reference Material (CRM) of the International Atomic Energy Agency (IAEA) IAEA H-4 (animal muscle) weighing about 100 mg were treated and analyzed in the same conditions as thyroid samples to estimate the precision and accuracy of results. The content of Ca, Cl, I, K, Mg, Mn, and Na were determined by INAA-SLR using a horizontal channel equipped with the pneumatic rabbit system of the WWR-c research nuclear reactor (Branch of Karpov Institute, Obninsk). Details of used nuclear reactions, radionuclides, gamma-energies, spectrometric unit, sample preparation, and the quality control of results were presented in our earlier publications concerning the INAA-SLR of ChEs contents in human thyroid [27,28], scalp hair [51], and prostate [52,53].
A dedicated computer program for INAA-SLR mode optimization was used [54]. All samples for ChEs analysis were prepared in duplicate, and mean values of ChEs contents were used in final calculation. Using Microsoft Office Excel software, a summary of the statistics, including, arithmetic mean, standard deviation of mean, standard error of mean, minimum and maximum values, median, percentiles with 0.025 and 0.975 levels was calculated for ChEs contents in two groups of tissue adjacent to TBN and TMN. Data for “normal” thyroid were taken from our previous publications [42- 47]. The difference in the results between two groups of samples “adjacent to TBN” and “adjacent to TMN”, as well as between “normal” and “adjacent to TBN and TMN combined” was evaluated by the parametric Student’s t-test and non-parametric Wilcoxon- Mann-Whitney U-test.
Results
Table 1 presents certain statistical parameters (arithmetic mean, standard deviation, standard error of mean, minimal and maximal values, median, percentiles with 0.025 and 0.975 levels) of the Ca, Cl, I, K, Mg, Mn, and Na mass fraction in thyroid intact tissue samples of two groups “adjacent to TBN” and “adjacent to TMN”. The ratios of means and the comparison of mean values of Ca, Cl, I, K, Mg, Mn, and Na mass fractions in pair of sample groups such as “adjacent to TBN” and “adjacent to TMN” is presented in Table 2. Table 3 depicts certain statistical parameters (arithmetic mean, standard deviation, standard error of mean, minimal and maximal values, median, percentiles with 0.025 and 0.975 levels) of the Ca, Cl, I, K, Mg, Mn, and Na mass fraction in thyroid tissue adjacent “TTA” to TN (two groups “adjacent to TBN” and “adjacent to TMN” combined). The ratios of means and the comparison of mean values of Ca, Cl, I, K, Mg, Mn, and Na mass fractions in pair of sample groups such as normal thyroid tissue “NT” and “TTA” is presented in Table 4.
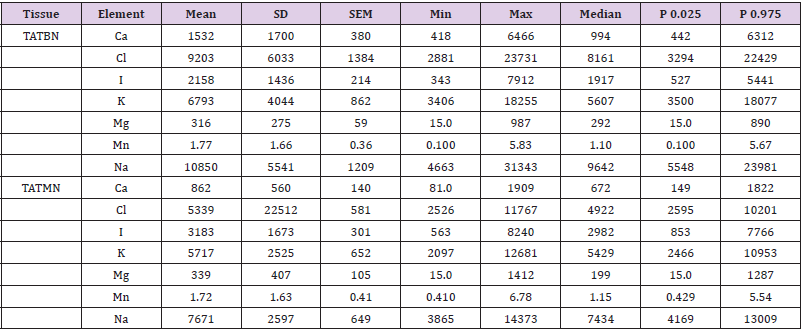
Table 1: Some statistical parameters of Ca, Cl, I, K, Mg, Mn, and Na mass fraction (mg/kg, dry mass basis) in thyroid tissue adjacent to thyroid benign (TATBN) and malignant (TATMN) nodules.
Note: M: Arithmetic Mean, SD: Standard Deviation, SEM: Standard Error of Mean, Min: Minimum Value, Max: Maximum Value, P 0.025: Percentile with 0.025 Level, P 0.975: Percentile with 0.975 Level.
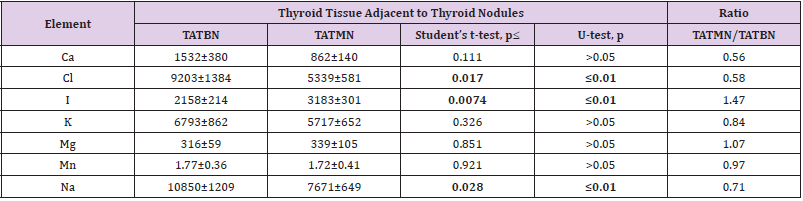
Table 2: Some statistical parameters of Ca, Cl, I, K, Mg, Mn, and Na mass fraction (mg/kg, dry mass basis) in thyroid tissue adjacent to thyroid benign (TATBN) and malignant (TATMN) nodules.
Note: M: Arithmetic Mean, SEM: Standard Error of Mean, Statistically significant values are in bold.
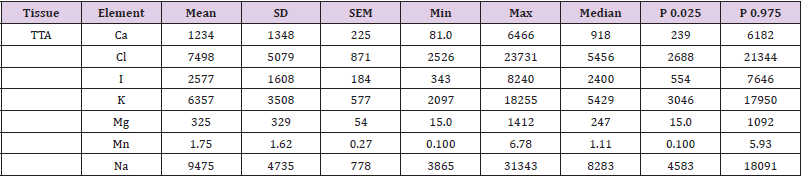
Table 3: Some statistical parameters of Ca, Cl, I, K, Mg, Mn, and Na mass fraction (mg/kg, dry mass basis) in in Thyroid Tissue Adjacent (TTA) to thyroid benign and malignant nodules (combined).
Note: M: Arithmetic Mean, SD: Standard Deviation, SEM: Standard Error of Mean, Min: Minimum Value, Max: Maximum Value, P 0.025: Percentile with 0.025 level, P 0.975: Percentile with 0.975 level.
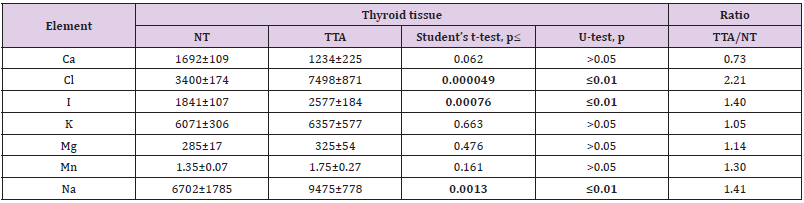
Table 4: Differences between mean values (MSEM) of Ca, Cl, I, K, Mg, Mn, and Na mass fraction (mg/kg, dry mass basis) in Normal Thyroid (NT) and Thyroid Tissue Adjacent to thyroid benign and malignant nodules (TTA).
Note: M: Arithmetic Mean, SEM: Standard Error of Mean, Statistically significant values are in bold.
Discussion
As was shown before [27,28,51-53] good agreement of the Ca, Cl, I, K, Mg, Mn, and Na contents in CRM IAEA H-4 samples analyzed by INAA-SLR with the certified data of this CRM indicates acceptable accuracy of the results obtained in the study of “adjacent to TBN”, “adjacent to TMN”, “NT”, and “TTA” groups of thyroid tissue samples presented in Tables 1-4. From Table 2, it is observed that in thyroid tissue adjacent to TMN the mass fraction of I is 1.47 time higher while mass fractions Cl and Na 42% and 29%, respectively, lower than in thyroid tissue adjacent to TBN. In a general sense Ca, K, Mg, and Mn contents found in the “adjacent to TBN” and “adjacent to TMN” groups of thyroid tissue samples were similar (Table 2). It allowed combine data obtained for two groups for the purposes of finding a common ChEs composition of TTA to TN and improving statistical characteristics of results for this group of samples (Table 3). From obtained results it was found that the common characteristics of thyroid tissue adjacent to TBN and TMN were elevated levels of Cl, I, and Na, which overdrew those in “normal” thyroid approximately in 2.2, 1.4, and 1.4 times, respectively (Table 4). Thus, if we accept the ChEs contents in “normal” thyroid glands as a norm, we have to conclude that with a nodular transformation the Cl, I, and Na contents in thyroid intact tissue adjacent to TN significantly changed.
Characteristically, elevated or reduced levels of ChEs observed in thyroid nodules are discussed in terms of their potential role in the initiation and promotion of these thyroid lesions. In other words, using the low or high levels of the ChEs in affected thyroid tissues researchers try to determine the role of the deficiency or excess of each ChEs in the etiology and pathogenesis of thyroid diseases. In our opinion, abnormal levels of some ChEs in TN could be and cause, and also effect of thyroid tissue transformation. From the results of such kind studies, it is not always possible to decide whether the measured decrease or increase in ChEs level in pathologically altered tissue is the reason for alterations or vice versa. According to our opinion, investigation of ChEs contents in thyroid tissue adjacent to TN and comparison obtained results with ChEs levels typical of “normal” thyroid gland may give additional useful information on the topic because these data show conditions of tissue in which TN were originated and developed.
Chlorine and Sodium
Cl and Na are ubiquitous, extracellular electrolytes essential to more than one metabolic pathway. In the body, Cl and Na mostly present as sodium chloride. Therefore, as usual, there is a correlation between Na and Cl contents in tissues and fluids of human body. Because Cl is halogen like I, in the thyroid gland the biological behavior of chloride has to be similar to the biological behavior of iodide. The main source of natural Cl for human body is salt in food and chlorinated drinking water. Environment (air, water and food) polluted by artificial nonorganic Cl-contained compounds, for example such as sodium chlorate (NaClO3), and organic Cl-contained compounds, for example such as polychlorinated biphenyls (PCBs) and dioxin, is other source. There is a clear association between using chlorinated drinking water, levels NaClO3, PCBs and dioxin in environment and thyroid disorders, including cancer [55-59].
Thus, on the one hand, the accumulated data suggest that Cl level in thyroid tissue might be responsible for TMNs development. However, on the other hand, it is well known that Cl and Na mass fractions in human tissue samples depend mainly on the extracellular water volume [60]. TN and thyroid tissues adjacent to nodules can be more vascularized than normal thyroid. Because blood is extracellular liquid, it is possible to speculate that more intensive vascularization could be the reason for elevated levels of Cl and Na in thyroid tissue adjacent to TB and TMN. If that is the only case, the equilibrium between Cl and Na increases has to be, however, in comparison with “normal” thyroid the change of Cl level in adjacent tissue is significantly higher than change of Na level. Thus, it is possible to assume that an excessive accumulation of Cl in thyroid tissue is involved in TBN and TMN etiology.
Iodine
To date, it was well established that iodine excess has severe consequences on human health and associated with the presence of TBN and TMN [4-8,61-64]. In present study elevated level of I in thyroid tissue adjacent to TBN and TMN was found in comparison with “normal” thyroid. Thus, on the one hand, it is likely that elevated level of I in thyroid tissue might be involved in the TN origination and development. On the other hand, however, elevated level of I in thyroid tissue adjacent to TN may explain by unusually intensive work of this tissue. Compared to other soft tissues, the human thyroid gland has higher levels of I, because this element plays an important role in its normal functions, through the production of thyroid hormones (thyroxin and triiodothyronine) which are essential for cellular oxidation, growth, reproduction, and the activity of the central and autonomic nervous system. As was shown in our previous study, TBN and, particularly, TMN transformation of thyroid gland is accompanied by a significant loss of tissue-specific functional features, which leads to a significant reduction in I content associated with functional characteristics of the human thyroid tissue [43-47]. Because the affected part of gland reduced productions of thyroid hormones, the rest “intact” part of thyroid tries to compensate thyroid hormones deficiency and work more intensive than usual.
Limitations
This study has several limitations. Firstly, analytical techniques employed in this study measure only seven ChEs (Ca, Cl, I, K, Mg, Mn, and Na) mass fractions. Future studies should be directed toward using other analytical methods which will extend the list of ChEs investigated in thyroid tissue adjacent to TN. Secondly, the sample size of TBN and TMN group was relatively small and prevented investigations of ChEs contents in this group using differentials like gender, functional activity of nodules, stage of disease, and dietary habits of patients with TN. Lastly, generalization of our results may be limited to Russian population. Despite these limitations, this study provides evidence on some ChEs level alteration in thyroid tissue adjacent to TN and shows the necessity to continue ChEs research of TN.
Conclusion
In this work, ChEs analysis was carried out in the thyroid tissue adjacent to TBN and TMN using INAA-SLR. It was shown that INAA-SLR is an adequate analytical tool for the non-destructive determination of Ca, Cl, I, K, Mg, Mn, and Na content in the tissue samples of human thyroid in norm and pathology. I was observed that in thyroid tissue adjacent to TMN the mass fraction of I is 1.47 time higher while mass fractions Cl and Na 42% and 29%, respectively, lower than in thyroid tissue adjacent to TBN. The common characteristics of thyroid tissue adjacent to TBN and TMN were elevated levels of Cl, I, and Na, which overdrew those in “normal” thyroid approximately in 2.2, 1.4, and 1.4 times, respectively and similar contents of Ca, K, Mg, and Mn. Thus, from results obtained, it was possible to conclude that the role of ChEs in etiology and pathogenesis of TBN and TMN is similar and exessive accumulation of Cl and I in thyroid tissue may be involved in the TN origination and development.
For more Articles on: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.