Is using Dynamic Distant Direct Ophthalmoscope Refraction an Alternative to Cycloplegic Refraction in Children? – A Comparative Study
Introduction
Accommodation of the eye is a function that involves a stimulus, communication of the signals in the system, the neurological changes in the ciliary muscle, and the resultant response [1]. The ciliary muscle contraction and relaxation play an active role in both stimulating and relaxing accommodation [2]. Accommodation is dynamic in children. The amplitude of accommodation slowly decreases as age increases. This factor needs consideration to measure refractive errors in children. Several earlier studies had shown that lack of cycloplegia led to an overestimation of myopia or a gross inaccuracy in estimating hyperopia and emmetropia in children. The recommended dose was 1% cyclopentolate three to four drops in dark irises children for an adequate cycloplegic effect [3]. It was observed on many instances children after undergoing cycloplegic refraction for the first time were reluctant to return for the follow-up visits due to the discomfort caused by cycloplegia. But cycloplegic refraction is the only objective method to measure the total refractive status of the eye without the influence of accommodation to date. Hence an alternate objective technique to estimate the amplitude of accommodation and the complete refractive error of the eye by the DDDO method and the gold standard cycloplegic refraction were compared.
Materials & Methods
A prospective observational cohort study was conducted in a school by an experienced blinded examiner. The subjects were between the ages of 5 to 7 years, without previous refractive errors, binocular vision anomalies, and other ocular defects from a semiurban, middle-class population. one hundred and ten children were selected by cluster simple random sampling, out of which ten children parents did not give consent owing to side effects of cycloplegia. As this age group has the active accommodative ability, conducting cycloplegicrefraction becomes mandatory and hence was selected for the study. The study followed the tenets of the Declaration of Helsinki and got approved by the Institutional ethics committee. We obtained parental consent after explaining the procedure alongside the possible side effects of the cycloplegic drug. Cycloplegic refraction followed the comprehensive eye examination, after instilling 1% cyclopentolate twice fifteen minutes apart between the instillations [4].
The following week the same children underwent DDDO refraction. DDDO refraction is shining direct ophthalmoscope light on the subject’s eyes from a 1- meter distance and noting the fundal glow emitted from the subject’s eyes. The presence of a superior crescent glow indicates the unaccommodated state of the eyes. An inferior crescent glow indicates the accommodated phase of the eyes based on the photorefraction principle [5]. The examiner performed the procedure after fully correcting their refractive error and fixing the ophthalmoscope at “0” dioptres all along. DDDO refraction was performed by initially instructing the child to fixate at a distance target at 6 meters. After noticing a superior crescent, the child had to fixate on an N8 notation letter at a 40cm distance. The expected glow was an inferior crescent for a near target affirming accommodated state of the eyes. The examiner slowly moved the target towards the child until a complete neutralization was appreciated. The distance of the chart from the child’s eyes where complete neutralization occurred was recorded in centimeters and converted to dioptres.
The starting point for the routine distance objective refraction was to place the dioptric value equal to the amplitude of accommodation in front of both eyes to nullify the accommodative effort. On completion of the distance refraction, the dioptric value after deducting the working distance power and the amplitude of accommodation was considered the total refractive error. For example, a child having neutralization of DDDO reflex at 10cm has 10.00Ds amplitude of accommodation. The child then fixates a distant target at 6 meters with a +10.00Ds in the trial frame to nullify the accommodative component. The +10.00Ds need deduction from the final neutralized power after completing the routine distance objective refraction to obtain the total refractive status of the child. Only the left eye spherical equivalent values of both cycloplegic refraction and the DDDO refraction was taken for analyses purpose.
Statistics
Data was entered in MS Excel. To confirm the type of distribution normality test using the Shapiro-Wilk test in SPSS 17.0 was done. The limits of agreement (LOA) between the two different methods of measurement (Cycloplegic refraction and DDDO refraction) were found using Bland Altman plots, which defined LOA = mean difference ± 1.96 x standard deviation of the differences between two methods. SPSS 17.0 was used to fit the data and for graphical representation.
Results
The study included 100 children with 100 eyes. Only the left eye was analyzed. Out of 100 children, 56 were females and 44 were males. The mean age of the cohort was 6.01 ± 0.52 years. The mean refractive error measured through cycloplegic refraction was 0.74D ± 0.234 (range -0.25 - 1.25, 95% CL 0.046D). The mean refractive error measured through DDDO refraction was 0.83D ± 0.238 (range 0.00 - 1.25, 95% CL 0.047D). A mean difference of 0.09D between cycloplegic refraction and the DDDO method was observed. The mean spherical equivalent of cycloplegic refraction and DDDO refraction values along with upper and lower limits is presented in (Figure 1). As normal distribution was absent, a Wilcoxon Signed Rank test revealed a statistically significant difference between the methods with p = 0.00 (95% CL 0.062 - 0.125) though it was not clinically significant. The number of subjects with refractive error difference between the cycloplegic and DDDO method is shown in (Figure 2). Bland Altman’s analysis found the limits of agreement between Cycloplegic and DDDO refraction. The mean difference between the two methods was 0.091 (CI 0.52, -0.34), as presented in (Figure 3). The refractive error difference did not exceed ±0.50D in either of the approach. The DDDO method showed a difference of +0.25D more than the cycloplegic method up to +0.75D while the lattershowed a difference of +0.25D from +0.87D onwards though neither are clinically significant.
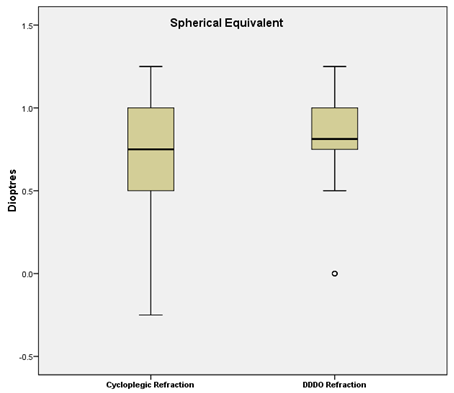
Figure 1: The mean spherical equivalent refractive values with upper and lower limits for both the methods.
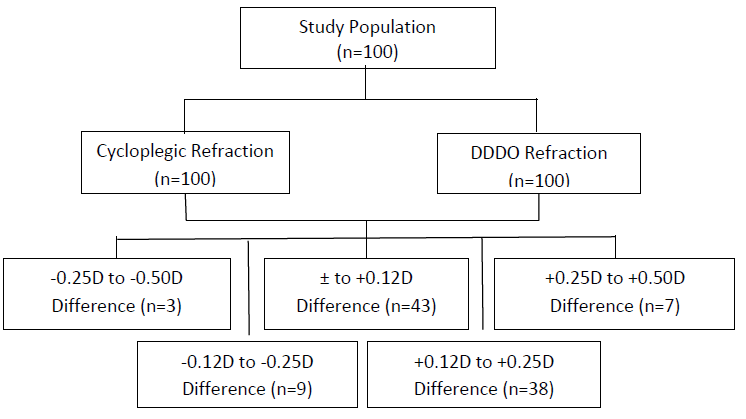
Figure 2: The flow chart of net refractive errors difference between two methods.
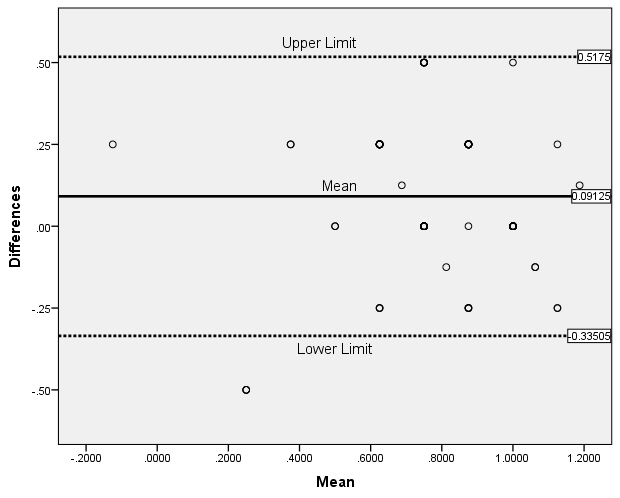
Figure 3: Bland altmann plot between the cyclopegia and DDDO refraction.
Discussion
An alternate objective technique to estimate the amplitude of accommodation and the complete refractive error of the eye by the Dynamic Distant Direct Ophthalmoscopy (DDDO) method was conceptualized and compared with the gold standard cycloplegic refraction among young children. It demonstrated good reliability as the limits of agreement between the methods were excellent as shown in (Figure 3) with a mean refractive error difference of 0.09D between the methods. Though there was a statistically significant difference between the methods, as the difference was only 0.09D, there was no clinical significance reinstating the agreement between the methods. DDDO method is much quicker and can be performed simultaneously in both eyes as opposed to cycloplegic refraction. Thirteen percent of the subjects showed a difference of +0.25D more by cycloplegic refraction than DDDO refraction. Only 10% of the subjects had a difference of ±0.50D in comparison with cycloplegic refraction. The DDDO refraction showed a difference of ± 0.25D more than cycloplegic refraction in 39% of subjects and was the same as cycloplegic in 38% of subjects.
The ±0.25Ds difference with the DDDO method can be attributed to the extraocular muscle tone, as this helps to maintain the fusion even after achieving complete accommodation due to proximal vergence which is absent in cycloplegic refraction. An earlier study, [5] comparing DDDO and dynamic retinoscopy proved to be correlating with each other in measuring the accommodation in children. This study further measured the total refractive error in children by comparing the DDDO refraction with the gold standard cycloplegic refraction. The box and whisker plot in (Figure 1) adequately represents the efficiency of the novel DDDO refraction method in comparison to cycloplegic refraction where none of the subjects had a spherical equivalent towards the myopic value emphasizing the adequacy in diagnosing uncorrected hyperopia, active accommodative influence, etc., The prevalence of hypermetropia in India between 3 to 18 years was 2.6% and 4.6% among the urban population [6,7].
Similarly, the prevalence of non-strabismic binocular vision anomalies among school children in southern India was 25.1% between the 7 to 12 years age group [8]. Vision screening in school children and the importance of earlydiagnosis to prevent reversible blindness were proven adequately in many earlier studies [9]. An earlier study [8] stated the importance of school screening for children aged 5 to 16 years to effectively diagnose and manage anomalies such as refractive errors, amblyopia, binocular vision, and color vision to improve the overall quality of these children [10]. All of these involve cycloplegic refraction for a precise diagnosis. Since carrying out cycloplegic refraction is long-winded for the examiner and causes distress to the child in a screening program, an alternate quick and efficient method was experimented with to combat the drawback.
The study did not compare the two different methods in anisometropic and myopic subjects. Since the novel DDDO refraction is a binocular procedure, monocular assessment is necessary in anisometropic cases for precise diagnosis. Despite performing monocularly in anisometropes, the technique will be fast and devoid of any after-effects of cycloplegic eye drops. The accuracy of this requires to be studied further. In addition, in myopic eyes, as the far point is at a closer distance, the efficiency of this novel procedure demands a further investigation of the same.
Conclusion
DDDO is a quick and easy method that can be employed to measure the total refractive error in patients suspected of an active accommodative mechanism as in children, uncorrected hyperopes, etc., instead of cycloplegic refraction. This study affirms the same since the gold standard cycloplegic refraction and the novel DDDO refraction method shows good agreement. DDDO method is swift and does not have any after-effects similar to that of cycloplegia like blurred near vision, nausea, etc. It is an effective alternative, especially in screening programs.
For more Articles on: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.