Low Cost CPAP for the Developing World
Introduction
The application of Continuous Positive Airway Pressure (CPAP) to the spontaneously breathing infants is a recognised therapeutic intervention for respiratory distress of the newborn, as well as bronchiolitis and pneumonia in the infant. It has been shown to be safe and to reduce the need for mechanical ventilation [1]. It may be applied through intranasal prongs or a nasal mask, with pressure generated by an upstream mechanical ventilator, or by downstream immersion of an exiting tube under required depths of water (Figure 1). In either case, the gases are usually supplied from bottled containers and, therefore, the mixture is likely to be dry and cold. Inhalation of ‘dry’ gas reduces the flow of mucous in the airways by interfering with the function of cilia and by drying secretions [2]. Inflammation may follow, with reduction of lung capacity, compliance and oxygenation [3]. In adults, such interference with flow of secretions has been demonstrated within 10 minutes of application [4]. Inhalation of cold gas has long been known to reduce muco-ciliary action [5]. Within the airways, Inhaled gas is heated and humidified to equilibrium with surrounding tissue, but this process takes energy. Dawson et al suggest that 1-2% of the infant’s energy consumption on the first day of life could, per hour, be expended on cold and dry gas [6].
Furthermore, they emphasise that oxygen consumption increases with the temperature gradient between child and environment. Inhaled gases can be heated and humidified before application but the apparatus is expensive. For example, in Australian dollars the single-use unit which humidifies the inhaled gas costs around $120 but its permanent heating base costs around $3600. To these costs are added those of single-use nasal prongs ($24) and gas supply. A standard 10 L tank costs around $260. If gas flows at 6 L/min, it will be emptied by 6 hours costing about $12 per day (Figure 1). Though the cost of refilling would appear to be minimal, third world budgets are limited, and gas re-supply often not guaranteed. Therefore, the use of small pumps that can entrain air at room temperature and humidity and deliver it at a rate to generate sufficient CPAP may be of advantage in developing world hospitals. The basic gas would be room air and the CPAP, by itself, may increase oxygenation to desired levels (Figure 2). If added oxygen is needed, it can be entrained into the inspiratory side of the apparatus, at the level of the nasal prongs, or further back in the tubing. If desired, inspired gas can be warmed by immersing tubing in warmed water bathes before it enters the nares. Pressure within the tubing, and thus CPAP, would be generated by the ‘fish tank pump’, supplemented by hydrostatic pressure associated with the depth of immersion of the exiting tubing beneath water in a nearby container.
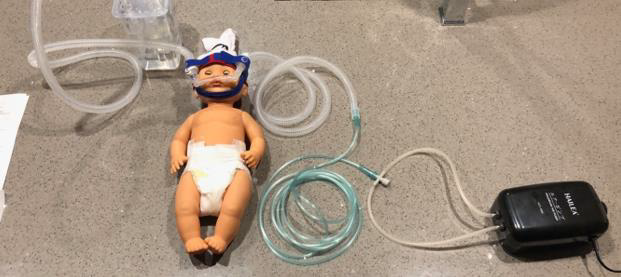
Figure 1: CPAP.

Figure 2: High Flow.
To reduce the loss of pressure at the nostrils though any gap surrounding the nasal prongs, the size of the gap was reduced by inserting the prongs through appropriately sized holes cut into non-damaging adhesive tape which was applied across the nostrils. In Bangladesh, we aimed to examine the usefulness of small pumps otherwise designed for aquaria, fitted with plastic tubing acquired from hardware shops, at a total cost of at a total cost of $26. CPAP was applied to noses with standard a Hudson Nasal Prong cannula, costing $24 each. Ethical approval was given by governance of Shishu Children’s Hospital, Mymensingh Community Hospital and Joyramkura Hospitals, Bangladesh. Parental approval was secured for each application of the apparatus.
Method
We employed Hailea ACO 6604 Air pumps with twin outlets each delivering approx. 4.5L/min, for a total of 9L/min. The prongs were applied through holes cut in underlying Duoderm to minimise escape of gas from the nares . The apparatus was held in place in front of the face by Velcro attachment to a knitted cap or a Canberra Hat (Figure 1). The exiting tube was submersed below water in a cheap container with depth measured by an affixed tape. Progress was monitored by recordings of Oxygen Saturations levels (SpO2), Heart Rate (HR) and Respiratory Rate (RR).
Results
21 infants with respiratory distress associated with bronchiolitis and pneumonia were recruited (Figure 3). The average weight was 2.900 Kg. Before the application of ‘fish tank CPAP’, respiratory support had comprised the application of supplemental oxygen via small bore nasal tubes. Overall, with CPAP between 6-7 cm/ H2O, there was a mean increase in SpO2 levels of 16.76%, a mean decrease in RR of 21.2 breaths per minute and a mean decrease in HR 17.52 per min (Table 1). The average time on CPAP was 16.76 hours. Reduction of RR was noted within several hours by some. No complications were noted. One child, however, succumbed to overwhelming sepsis.

Figure 3: CPAP in use in Mymensingh Children’s Ward.
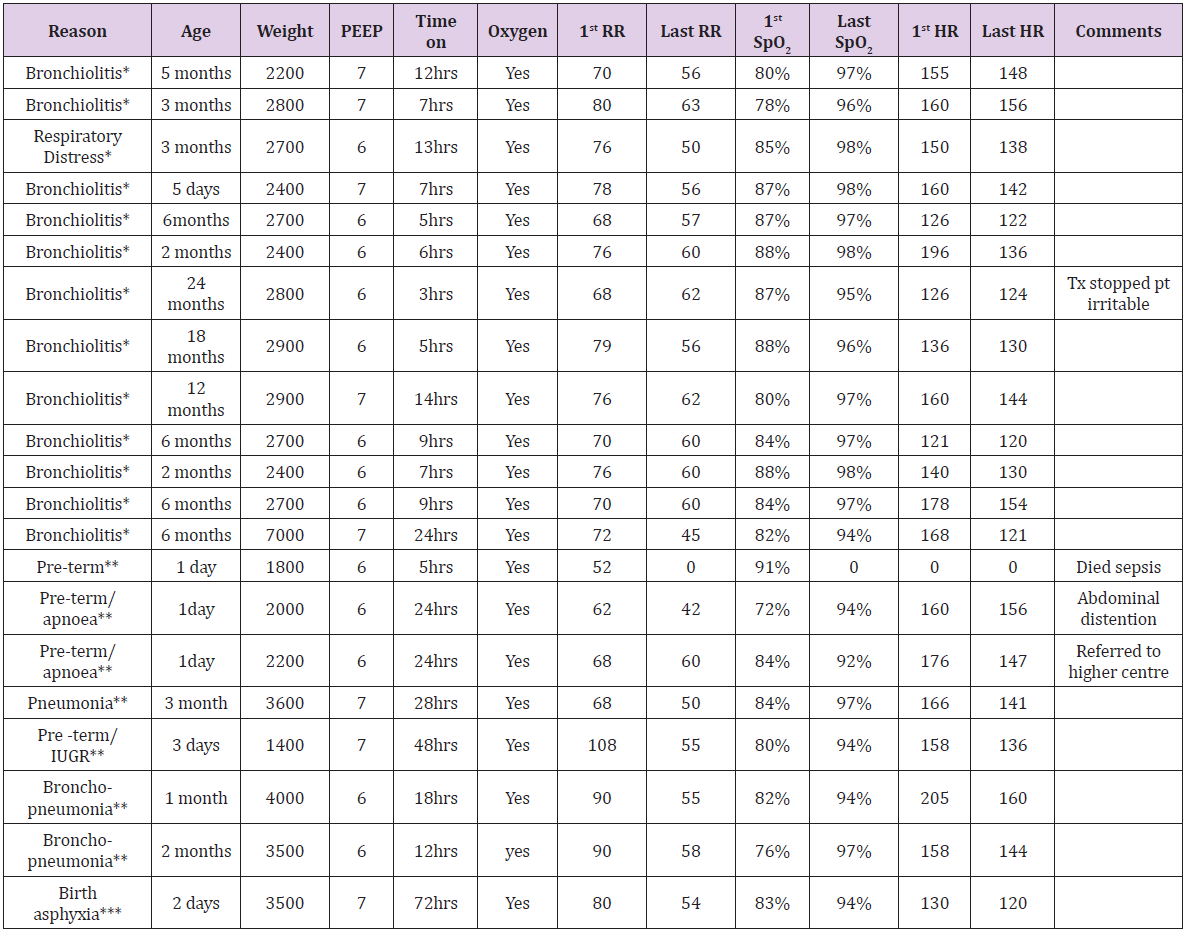
Table 1: Neonate and Infant data collected from 3 Bangladeshi Hospitals.
Note: *Shishu Childrens Hospital, **Mymansingh Community Hospital, ***Joyramkura.
Conclusion
The ‘fish tank’ apparatus can support ventilation and improve oxygenation in infants with respiratory distress in resource poorsettings, dramatically reducing costs. We used expensive nasal prongs but Chisti et al have demonstrated, also in Bangladesh, that inexpensive ‘high flow’ tubing with In inbuilt nasal prongs can be modified to produce CPAP by immersing one limb of the tubing beneath water (Figure 2) [7]. We have not yet established how long the ‘fish tank’ pumps will continue to work but experience suggests continued function for many months. Costs of replacement would be reduced by bulk buying. Anecdotally, ‘fish tank’ pumps have been trialled by one of the authors in Papua New Guinea and Madagascar. Indications have included severe pneumonia, bronchiolitis, apnoea of prematurity, as well as neonatal respiratory distress. They have been demonstrated to be efficient but the busyness of the hospitals has, thus far, precluded sufficient documentation for publication. Our study is thus limited by lack of local resources including access to blood gas machines, as well as demands of service load. Nevertheless, in ‘fish tank’ or other small pumps would appear to offer the possibility of CPAP in resource poor settings.
For more Articles on: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.