A Cross-Sectional Study on the Acceptance of Covid-19 Vaccine
Background
Since the beginning of the 20th century, the world has witnessed several crises which are epidemic and pandemic in nature. In the year 1918-1920, the Spanish Flu is popularly known as Influenza occurred and affected about one-third of the world population. In the 21st century, the SARS outbreak occurred in 2003, the Middle East Respiratory Syndrome (MERS) outbreak occurred in 2015, and the latest recent novel (2019-2020) Coronavirus (COVID-19). All these are known to have negatively affected the world economy. The current pandemic COVID-19 is caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) (WHO, Cucinotta, et al. [1,2]). It is an acute respiratory infectious disease which was originated in Wuhan, China in December 2019, and swiftly become a global threat affecting 220 countries (WHO, Helmy [1,3]). As of September 2021, there are more than 219 million cases (infected persons) and more than 4.55 million deaths recorded worldwide (WHO) [1]. In the African continent, there were about 4% cases of mortality, and Nigeria having 193,000 cases and 2,480 deaths (Worldometer [4]).
The pandemic has resulted in a devastating impact globally, which prompted the limit to a movement among other restriction policies to contain the pandemic (Ilesanmi [5]), as most countries strategy was to lessen the transmission of the disease, especially by non-pharmaceutical interventions (NPIs), such as enforcing hands sanitization, face masks policy, travel restrictions, social distancing, and complete or partial lockdowns (Ilesanmi [6]). So far, these interventions have not been able to curtail the spread of the disease, but they are effective strategies to minimize the spread if properly adhered to. Medical technologies have been put in place to prevent and cure the disease; among are affordable, safe, and effective antiviral vaccines and drugs. Despite the high mortality rate in the world as a result of COVID-19, there were no approved antiviral drugs and vaccines to specifically fight against SARS-CoV-2 (Ilesanmi [7]) till the end of November 2020. As of December 2020, the US Food and Drug Administration (FDA) granted an Emergency Use Authorization for critically ill COVID-19 patients (FDA; Beigel, et al. [8,9]).
Nonetheless, the WHO recommended that this is not effective for COVID-19 but can only suppress the intensity of the disease (Rochwerg, et al. [10]). Vaccines are interventions effectively used to reduce disease’s high burden globally. They are usually reliable and cost-effective public health interventions for saving millions of lives (Rodrigues, et al. [11,12]) from polio, yellow fever, measles, etc. Following the trend of the SARS-CoV-2 in the second, third, and fourth quarters of 2020 (Wu, et al. [13]) and the global pandemic declaration by the WHO in March 2020 (Cucinotta, et al. [2]) public and private stakeholders including scientists and pharmaceutical organizations have resulted to developing vaccines (Coustasse, et al. [14]). It is pertinent to note that as of January 2021, at least 85 vaccines have been subjected to preclinical trial in animals, and 63 vaccines passed the test and were subjected to clinical development in humans.
From these 63 vaccines, 43 were approved for phase I; from these 43, 22 were approved for phase II; from these 22, 18 were approved for phase III; from these 18, 6 were finally approved for early use though later restricted; from these 6,2 vaccines were approved for total use though one vaccine has been neglected (Coustasse, et al. [14]). Pfizer-BioNTech’s (BNT162b2) and Moderna’s (mRNA-1273) mRNA vaccines were approved for use, but Pfizer-BioNTech’s (BNT162b2) was widely accepted. With the news about the approval of COVID-19 vaccines, there is a tendency that the high surge of disease transmission will be minimized (Omer, et al. [15]). Nonetheless, there are hindrances to achieving the general acceptability of the vaccines, among the hindrances are the issues surrounding individual perception regarding the vaccine which is influenced by the level of socio-economic factors of an individual (such as education, age, culture), source of information, personal encounter, among all (Omer, et al. [15,16]), and more rampant in Africa and Nigeria (Ilesanmi OS [7]).
Vaccine hesitancy was recognized by the WHO Strategic Advisory Group of Experts (SAGE) as a “delay in acceptance or refusal of vaccination despite the availability of vaccination services” (Huo, et al. [17]). With the introduction of new health interventions, there are uprising issues regarding the interventions. For instance, the polio vaccination program in northern Nigeria was not accepted because of the wrong teachings of Islamic clerics (Jegede, 2007). This experience was also recorded in Ghana where community members did not comply with the de-worming interventions (Dodoo, et al. [18]). The major factor that was responsible for these rejections was a result of the lack of clarification (misunderstanding) on the interventions (Febir, et al. [19]).
It is therefore obvious that peoples’ knowledge of any infectious disease influences their acceptability of the interventions (vaccines) provided for tackling such disease. The acceptability of vaccine intervention is determined by three major factors: convenience [relative ease of access to the vaccine; physical availability of the vaccine; affordability and accessibility to the vaccine (Ilesanmi, et al. [20]), confidence [faith in the safety and efficacy of the vaccine; faith in the dynamics of healthcare delivery system; and faith in the policymakers (Zimmer, et al. [21]), and complacency [this is connected with diseases that are low risk and may not necessarily require vaccine; hence there are more negative acceptance towards the intervention of such diseases (Olaimat [22]).
Studies were conducted on the acceptance of citizens to the usage of COVID-19 vaccine, among the studies are Olaimat, et al. [22] on knowledge and information sources about COVID-19 among university students in Jordan; Pogue, et al. [23]on the influence of attitudes regarding potential COVID-19 vaccination in the United States; Malik, et al. [24] on the determinants of COVID-19 vaccine acceptance in the United States; Lazarus, et al. [25] on a global survey of potential acceptance of a COVID-19 vaccine in the United States; Coustasse, et al. [14] on the challenge of COVID-19 and vaccine hesitancy in the United States must overcome; El-Elimat, et al. [26] on the cross-sectional study of acceptance and attitudes toward COVID-19 vaccines in France and Jordan. Furthermore, Huo, et al. [17] conducted a study on the knowledge and attitudes about the Ebola vaccine among the general population in Sierra Leone; Febir, et al. [19] on the community perceptions of a malaria vaccine in the Kintampo districts of Ghana; Solís, et al. [27] on the COVID-19 vaccine acceptance and hesitancy in low and middleincome countries in Asia, Africa, and South America, Russia; and Olapegba, et al. [28] on COVID-19 knowledge and perceptions in Nigeria; Ilesanmi, et al. [5]on the perception and practices during the COVID-19 pandemic in an urban community in Nigeria.
The majority of these studies were conducted with the use of online respondents; they employed a cross-sectional approach of methodology; multinomial and binary logistic regression was found to be a dominant test of data analysis. However, the studies were most prevalent in the developed countries while scarcity of such studies in developing countries and Nigeria in particular. Because the level of acceptance of COVID-19 vaccines and the perception of COVID-19 differs among citizens of different countries, this study examines the acceptance of Nigerians to the usage of the COVID-19 vaccine.
Methods
This study employed a descriptive cross-sectional study in Nigeria. No consent was obtained as the data were collected and analyzed anonymously. A cross-sectional survey-based study was conducted in June 2021. Amid the global pandemic, data was further gathered from social media platforms. Also, online social media platforms (Facebook, WhatsApp) were used to recruit respondents (Olapegba, et al. [20,28]). With the high level of internet penetration in Nigeria which stands at 51.4% based on the nation’s population (Statista [29]), it is therefore justified that more citizens will be able to participate in the study. Respondents were encouraged to share the e-questionnaire with friends, contacts, or acquaintances. A sample of (n = 38) was employed to improve the clarity of the survey items. Data from the pilot sample was jettisoned as it was not used further for analysis. Categorical variables were presented as numbers and percentages, while continuous variables were presented as median [interquartile range].
The univariate analysis was performed using an independent Mann–Whitney U test for continuous variables and Chi-square test for categorical variables as appropriate. For analysis, responses to the attitudes section were combined. For example, both responses “strongly agree” and “agree” were combined in one category and both responses “strongly disagree” and “disagree” in one category. Before analysis, the independence of variables was analyzed using a correlation matrix. No multicollinearity was detected among predictor variables. To identify the factors that affect the acceptance of COVID-19 vaccines by Nigerians, binary and multinomial logistic regression were employed. The significance level [p <.05] was employed for affirming statistical decisions. Concerning the binary logistic regression model, the respondents were dichotomized as acceptable or not acceptable. The odds ratio (OR) values and the confidence intervals (95% CI) were calculated. The analysis was conducted using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL) version 23.
Results
Demographics
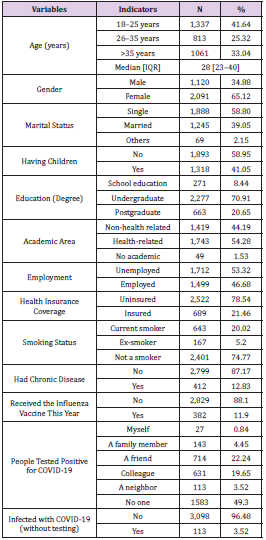
Table 1: Demographic details of study respondents (n = 3,211).
Note: Source: Authors’ work (2021)
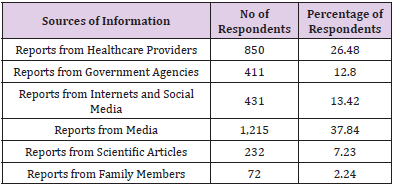
Table 2: Sources of information regarding COVID-19 vaccines.
Note: Source: Authors’ work (2021)
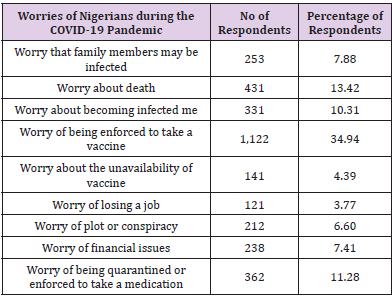
Table 3: Worries of Nigerians during the COVID-19 Pandemic.
Note: Source: Authors’ work (2021)
The study received 3291 submissions of which 3211 were complete and included in the final analysis. The median age of respondents was 28 years old and more than half of them were females (65.12%). More than half of the respondents were single (58.80%). About 70.91% had an undergraduate degree and more than half (54.28%) with health-related educational backgrounds. Besides, 46.68% of the respondents were employed and only 12.83% had chronic diseases (See Table 1). Less than 12% of the respondents received the influenza vaccine this year. About 0.84% of the respondents reported that they had tested positive for COVID-19. However, a minimal number of respondents (3.52%) stated that they might have been infected with COVID-19, but they did not verify it by laboratory test. As revealed in Table 2, about half (37.84%) of the respondents believed in the media reports while another significant percentage (26.48%) believed in the healthcare providers as a source of information about COVID-19 vaccines. About 13.42%, 12.8%, and 7.23% of the respondents believed the reports sourced from the internet and social media, reports from agencies, and reports from scientific articles respectively. During the COVID-19 pandemic, the respondents were worried about different issues (See Table 3). The major issue was the fear of being enforced to take a vaccine (34.94%), which is higher than the fear of death (13.42%) and fear of being quarantined or enforced to take a medication (11.28%). The fact that there are a sizeable number of respondents that have fear of taking vaccines, therefore, the acceptance of vaccines can be a bit negative. Hence, there is a need for serious sensitization among the general public.
Acceptance for COVID-19 Vaccines
As earlier stated that there are a considerable number of respondents that have fear of taking vaccines, which may pose threat to the acceptability of the vaccines; Table 4 depicts the multivariate analysis (binary logistic regression) of independent factors that predicted the level of acceptance. The study found that older age categories (>35 years old) may not accept COVID-19 vaccines compared to younger age categories (OR = 0.487, 95 CI% = 0.328– 0.675, p< .001). Also, employed respondents (OR = 0.653, 95CI% = 0.516– 0.836, p <.001) may not accept COVID-19 vaccines compared to unemployed respondents. Respondents that believed in the conspiracy dynamics of COVID-19 pandemic (OR = 0.613, 95 CI% = 0.467–0.811, p< .001) and those that did not believe in the information (OR = 0.382, 95 CI% = 0.294–0.511, p< .001) may not accept the vaccine. On the other hand, males were more likely to have acceptance for COVID-19 vaccines (OR = 2.589, 95 CI% = 1.745–3.486, p< .001) compared to females.
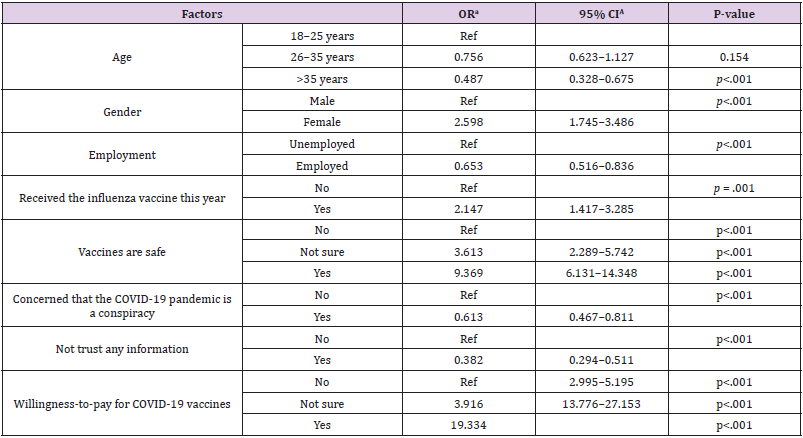
Table 4: Predictors of acceptance for COVID-19 vaccines.
In addition, respondents who took the influenza vaccine this year were more likely to accept COVID-19 vaccines compared to those who did not take the influenza vaccine (OR = 2.147, 95CI% = 1.417–3.285, p = .001). Furthermore, respondents who stated that vaccines are safe in general were more likely to accept taking COVID-19 vaccines compared to those who stated that vaccines are not safe (OR = 9.369, 95CI% = 6.131–14.384, p <.001). Moreover, respondents who expressed their willingness to pay for COVID-19 vaccines have a high tendency of accepting the COVID-19 vaccines than those that did not show their willingness to pay (OR = 19.334, 95CI% =13.776–27.153, p <.001). The acceptance group will be dominated by people who did not believe in the conspiracy notion of COVID-19. Those who believe that vaccines are unsafe have the same ideology as those who are not willing to pay for the vaccine whenever it is available.
Discussion
This study examined the acceptance of Nigerians to the usage of COVID-19 vaccines and the factors influencing the level of acceptance. It was needed to unravel the doubtfulness regarding COVID-19 and its’ vaccines among the general public. The doubtfulness regarding the COVID-19 vaccine could reduce the efficacy of COVID-19 vaccines as soon as they are widely available nationwide (Olapegba, et al. [28]). Regarding the comparison of findings of this present study with the findings of previous studies on public acceptance and willingness to receive the COVID-19 vaccines nationwide, Nigeria is among the lowest countries with sufficient availability as the first batch of Oxford/AstraZeneca shots landed 2nd March 2021 and acceptance stands at only 1.23% as of 4th September 2021. While Africa as a whole only has 3% of its population vaccinated, Seychelles remains the highest vaccinated in Africa with 74.1% and Nigeria sitting at the 36th vaccinated even in Africa. From a study on the acceptance of COVID-19 vaccine across fifteen surveys covering Africa, Asia, Russia, South America, Russia, and the United States which targeted a total of 44,260 participants, it was revealed that there is a significantly higher level of acceptance towards taking COVID-19 vaccines with mean of 80.3%; median of 78%; range 30.1% in African countries, while mean of 64.6% and 30.4% in the United States and Russia respectively (Solís [27]).
Moreover, most western countries report relatively higher public acceptance. The acceptability level of vaccinations in Nigeria was far lower than global averages (Ilesanmi, et al. [20]). This was based on 440 respondents, and it was revealed that many individuals (67.30%) were aware of the prospective COVID-19 vaccine. This corroborates with the studies of Sani et al. (2016); Wang et al. (2018) which found a positive relationship between education and health awareness. In this study, factors influencing the acceptance of COVID-19 vaccines were analyzed with logistic regression. It was revealed that younger respondents were more likely to accept COVID-19 vaccines; this does not agree with the findings of El-Elimat, et al. [22,26] which found higher acceptance among older age categories. This may be as a result of different age distribution, and the fact that a country may be dominated by some categories of people (based on age), literacy level, and other factors that may influence the awareness of prospective health interventions. It is pertinent to note that alternate mediums of information dissemination could be employed for health interventions.
Examples are conventional media such as Radio, Television, and non-traditional media such as Facebook (Abdelhafiz, et al. [30]). COVID-19 pandemic as with other previous pandemics is associated with feelings of fear, anxiety, and worries (Olaimat [22]). Nonetheless, people are not fearful of getting infected or transmitting the disease to others, but they experienced economic and societal concerns because of the measures that were embarked upon by the governments to minimize the pandemic and halt human-to-human transmission of the disease (Dodoo, et al. [18]). These measures entail the enforcement of social distancing, lockdowns, curfews, self-isolation, borders’ shutdowns, school and universities closures, quarantine, and travel restrictions (Ilesanmi [5]).
In this current study, fear of taking vaccines and fear of death were most prevalent within the Nigerian population. This agrees with the findings of Holingue, et al. [31] among the US adults population which found that anxiety and fears of getting infected and died as a result of COVID-19 were linked to the increasing mental distress. In the study of French, et al. [32], the acceptance of the COVID-19 vaccine among college students in South Carolina was identified to be influenced by the information obtained from scientists (83%), followed by healthcare providers (74%), and then health agencies (70%). Nevertheless, contrary to this present study, information was not popularly disseminated by pharmaceutical companies in Nigeria. In the study of El-Elimat, et al. [25] in France, vaccination hesitancy and acceptance toward HBV and MMR vaccines were better when parents were informed through their healthcare providers. This seems more efficient than information sourced from the internet or a third party. However, it should be clearly stated that no matter the source of information, such information must be properly screened before absorbed.
Conclusion
This study aimed to examine the acceptance of Nigerians to the usage of COVID-19 vaccines and the factors influencing the level of acceptance. It was necessitated because of the level of doubtfulness regarding COVID-19 and its’ vaccines among the general public. An online cross-sectional study was conducted, achieved by the use of an e- questionnaire which was administered to respondents (Nigerians) in a form of an online survey with some particular emphasis on the COVID-19 vaccine acceptance. A total of 3291 respondents completed the survey, but 3211 responses were valid for data analysis and reporting, and logistic regression analysis was employed for data analysis. The Nigerian public COVID-19 vaccines acceptance was fairly low in Nigeria. The educated male respondents are most likely to accept the usage of the vaccine. Similarly, respondents who believed that vaccines are generally safe and those who were willing to pay for vaccines, after becoming widespread, were more likely to accept the COVID-19 vaccines.
However, those above 35 years old and respondents who are employed were not likely to accept the vaccines except been mandated by the employers. Moreover, respondents that believed in the rumors surrounding the dynamics of COVID-19 as well as those that do not have assurance in any source of information regarding COVID-19 vaccines, may not accept the usage of the vaccine. It was concluded that the most reliable sources of information regarding the COVID-19 vaccines were reports from the media and reports from healthcare providers. Organized interventions are essential by the authorities of healthcare providers to minimize the levels of doubt regarding COVID-19 vaccines, and advance approaches general acceptance. Further studies should be carried out to assess the awareness campaigns organized by both public and private stakeholders.
Take home message: Studies, reports and life experiences have established that COVID-19 is real in the developed and developing countries; therefore, the transmission is inevitable. Since the impact of COVID-19 on human life is fast killing, there is a need to employ vaccine to reduce the impact on human health. The available vaccine have been tested and passed through various stages such that it is fit for use.
For more Articles on: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.