Characterization of Patients with Acute Appendicitis in the Elderly
Introduction
The first who drew attention to inflammation of the appendix cecal and gave it the name of acute appendicitis was Vidusenen 1561.1 In 1886 Kronlein performed the first appendectomy for apendicitis perforated the patient died. Later in 1887 T.G. Morton of Philadelphia performed the first successful appendectomy [1,2]. In Cuba, in 1893, Dr. Francisco Plá presented a presentation at the Society of Clinical Studies of Havana, about the first case of acute appendicitis, and it was in 1900 that Dr. Enrique Fortún performed the first appendectomy [1,2]. Acute appendicitis occurs in the elderly with a frequency between 5 and 10%. In those under 65 years of age, mortality is 0.2%, while in those over 65 years of age it is 4.6% [2,3]. Specifically in Cuba, the number of people aged 60 and over has varied from 11 .3% in 1985 to 20.4% in 2018 and 21.3% in 2020. In 2025, Cuba will be the oldest country in America [1]. Acute appendicitis in geriatric patients is a challenge for the surgeon, since this group of patients is always accompanied by comorbid conditions, so any delay in diagnosis and treatment significantly increases the already recognized high morbidity and mortality of abdominal sepsis in the elderly [4]. In accordance with the above , the American Society of Anesthesiology (ASA), presented a classification to define surgical risk, according to the functional limitations caused by coexisting diseases. It is important to point out that when comparing the mortality curves according to the ASA classification, it is concluded that postoperative mortality is more related to coexisting diseases than to chronological age [5]. In addition to this classification, it should be taken into account account that there is a progressive decline in the physiology of the elderly, in such a way that that the physiological reserve that is usually adequate for elective surgery may be insufficient when it comes to an emergency or a postoperative complication [6]. The diagnosis of acute appendicitis is essentially clinical. The Examination of the abdomen is performed by areas where there is less pain. Digital rectal examination should be performed routinely [7]. We must bear in mind that the symptoms are late and nonspecific and that the elderly have low sensitivity to pain and the febrile response is usually discreet [8]. An atypical clinical picture is common in elderly patients [9]. Sometimes it is difficult to establish a definitive diagnosis of acute appendicitis in the geriatric patient [10]. With the purpose of reduce complications and mortality from this disease, it is that the following work is carried out with the objective of characterize the behavior of acute appendicitis in adults in the “Enrique Cabrera” Hospital over a period of ten years.
Methods
An observational, descriptive longitudinal study was carried out retrospectively in the period between January 2011 and December 2020. The patients were studied from their admission until hospital discharge. Universe and sample. The universe was made up of all patients over 60 years of age who underwent surgery for acute appendicitis at the “Enrique Cabrera” General Teaching Hospital, with a total of 114 cases. It was not necessary to use a sampling method, nor to calculate the sample size since we refer to total number of patients over 60 years operated for acute appendicitis. Inclusion criteria. Patients older than 60 years intervened surgically for acute appendicitis. Data processing and analysis. patient information operated for acute appendicitis was obtained from the medical records of the General Surgery Service of the “Enrique Cabrera” Hospital and then transferred to a data collection form that was subsequently processed and analyzed with the Microsoft Office Excel 2010 program. The results were expressed through descriptive statistics in absolute frequencies, percentages and arithmetic mean Ethical parameters. The principles referring to the code of ethics in accordance with the Declaration of Helsinki. It was guaranteed security and confidentiality of the information, clarifying that the data derived from the research would be used for scientific purposes. The study was approved by the Hospital Ethics Committee.
Results
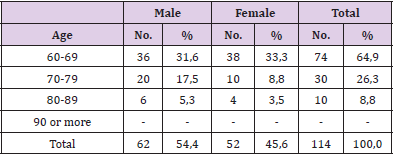
Table 1: Distribution of patients over 60 years operated.
Note: Sources: Information obtained from medical records.
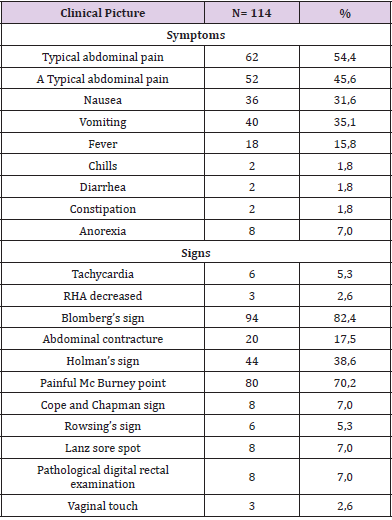
Table 2: Distribution according to clinical picture.
Note: Sources: Information obtained from medical records.
As can be seen in Table 1, the age group was comprised of between 60 and 69 years with 64.9%. The male sex was the one with the highest incidence with 54.4%. Abdominal pain was the symptom present in 100% of the patients. patients, typical abdominal pain prevailed in 62 of them (54.4%), only 18 had fever. There were 94 with positive Blomberg’s sign, 80 cases (70.2%) had a painful Mc Burney point, only six had tachycardia, all of which is shown in Table 2. Table 3 shows us that in the 100 leukograms recovered from the medical records, leukocytosis was observed in 78% of 78%. No, we were able to retrieve the results of fourteen leukograms in the medical records. In all cases where it was possible to perform computerized axial tomography, the diagnosis was positive. Most of the patients assessed preoperatively by the fitness classification of the American Society of Anesthesiology corresponded to ASAII 80 cases (70.2%), which is observed in Table 4. Table 5 shows that the most common anatomical-pathological diagnosis frequent was suppurative appendicitis in 74 patients 65.0%. In six of them confirmed appendiceal gangrene 5.2%.
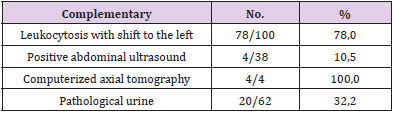
Table 3: Distribution of complementary.
Note: Sources: Information obtained from medical records.
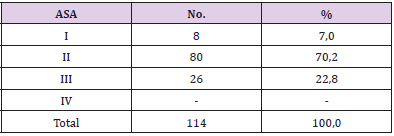
Table 4: Distribution according to physical status classification by the American Society of Anesthesiology.
Note: Sources: Information obtained from medical records.
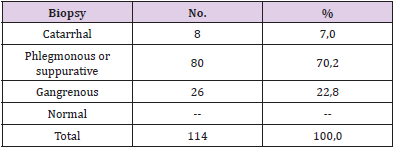
Table 5: Distribution according to anatomy-pathological stages of inflammation of the cecal appendix.
Note: Sources: Information obtained from medical records.
Discussion
Acute appendicitis occurred more frequently in patients aged between 60 and 69 years, which coincides with that reported by other authors [1,2]. The lower frequency in ages older than 69 years is related to appendicular atrophy due to the involution of the lymphoid tissues of the appendix [2,3]. In the study, the incidence of the disease prevailed in the sex masculine with respect to the feminine. In the reviewed literature, supports that from the sixth decade of life the difference with regarding sex, it ceases to manifest itself [2,7]. The physiological changes that occur with aging modify the functioning of each organ, an example of this is the perception of pain, which is usually less marked with increasing age, the same happens with fever, due to depression senile immune system called immunosenescence [2]. In our patients, the most important symptom was pain. abdominal, different from the younger ones, in which if the sequence of the appearance of pain, first visceral and then somatic.
When diarrhea or constipation is present in the clinical picture, as occurred in two patients in the study, it is related to pelvic or retroileal appendicitis where appendicitis, due to its unusual position near the rectum, generates said symptom [8,10,11]. On physical examination it was found that the signs considered cardinal for the diagnosis of acute appendicitis as they are the sign of Blomberg, painful Mc Burney point and others were manifested, but in a lower frequency than that presented in young people, which coincides with other studies reviewed [2,3,8,9]. The above is explained because the perception of pain decreases, due to The diseases Concomitant cardiovascular events that limit the cardiovascular response, such as increased heart rate. Regarding the laboratory tests, the leukogram reported an acceptable sensitivity to corroborate the suspected diagnosis of inflammatory process of the appendix. The use of abdominal ultrasound is not a routine indication for the diagnosis of acute appendicitis, but it was performed in most patients, as an aid to the differential diagnosis.
The anatomical-pathological study of the appendix showed advanced stages of acute appendicitis, suppurative in most of the 57 patients who underwent surgery. The rate of appendiceal perforation (including perforation and gangrene) was low in the study compared to other investigations reporting rates from 30% to 70% [2,9]. Perforation of the appendix is the single most important predictor of mortality and late diagnosis is the main cause of this. The most common postoperative complication was site infection. operative, which coincides with other studies such as that of González E. and others [12,13]. Study morbidity was low and mortality nil, other sources literature reports it below 1% [2]. In our study, showed a satisfactory postoperative evolution of the patients. Acute appendicitis is a disease that occurs in the elderly patient with attenuated symptoms due to involution of the lymphoid tissues of the appendix, in addition to the physiological changes that occur with aging, which they modify the functioning of each organ [14-16]. In 2025, Cuba will be the oldest country in America and the sagacity and experiences of our surgeons in the diagnosis of this disease, morbidity and mortality will be very low or zero [2].
Conclusion
Patients over 60 years of age who underwent surgery for acute appendicitis were predominantly male, between 60 and 69 years of age, with typical abdominal pain and classic signs of the disease. The suppuration phase of the appendix was mostly confirmed. A favorable evolution of the patients was observed.
For more Articles on: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.