Oral Hygiene Status and Practices Among Children Attend Dental Hospital in Dhaka City
Introduction
Good oral hygiene is an indicator for good body health. Oral diseases have been a persistent public health problem globally, with almost every individual experiencing poor oral health at least once in their lifetime [1,2]. Globally, poor oral hygiene occurring due to increasing plaque and calculus deposits with increasing age have been reported among children and adolescents. Only a minor proportion of school going children in Bangladesh has good oral hygiene compared to larger population among developed countries [3]. Poor oral hygiene not only affect the oral cavity but also a risk factor for initiation of many systemic diseases. Presence of dental plaque is an indicator of poor oral hygiene and if not treated properly can change into dental calculus which will further deteriorate the situation. Oral hygiene is a state of oral and related tissues and structures that contribute positively to physical, mental and social wellbeing and to the enjoyment of life possibilities by allowing an individual to speak, eat and socialize unhindered by pain, discomfort or embarrassment [4]. Dental plaque is a biofilm or mass of bacteria that grows on surfaces within the mouth. It is a sticky colorless deposit at first, but when it forms calculus, it is often brown or pale yellow. Dental plaque is also known as microbial plaque, oral biofilm, dental biofilm, dental plaque biofilm or bacterial plaque biofilm [5].
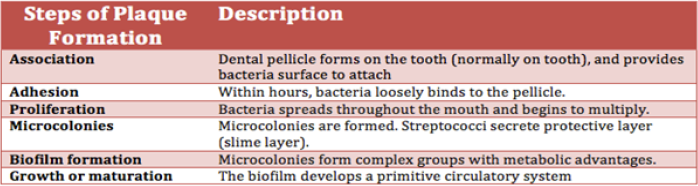
Plaque largely is made up of commensal species in the mouth. Dental plaque formations involve an ordered pattern of colonization by many different bacteria like Streptococcus mutans and other anaerobes include Fusobacterium and Actinobacteria which cause dental caries and periodontal diseases. Children who have dental caries in their primary dentition are more likely to have dental caries in permanent dentition. Permanent teeth erupt during the school age years, good dental hygiene and regular attention to dental caries are vital parts of health supervise [5]. Worldwide, approximately 2.3 billion people (32% of the population) have dental caries in their permanent teeth [6]. The WHO estimates that nearly all adults have dental caries at some point in time. In baby teeth it affects about 620 million people or 9% of the population [7]. They have become more common in both children and adults in recent years [8]. The disease is most common in the developed world due to greater simple sugar consumption and less common in the developing world [9]. A previous study reveals that in Bangladesh, children were affected most by dental caries than adults at age of 18 and 35 to 45 years in all socioeconomic groups [10]. The prevalence of dental caries is of great interest for long and is a principal subject of many epidemiological research carried out all over the world [10]. A limited survey was done with children, but real scenario was not reflected in Bangladesh regarding this crucial condition, actual data is not available. According to the health importance of dental caries, the aim of this study is to identify oral hygiene practices pattern and oral hygiene status among children.
Methods and Materials
Study Design
Cross sectional descriptive study was carried out. The study was conducted in Dhaka Dental College and Hospital, Mirpur-14. The study was conducted during the period of January 2019 to June 2019. The study population consisted of child patient whose age was 4 to 14 years, came for examination and treatment purpose in Dhaka dental college and hospital. Data was checked for the completeness and consistency on daily basis of data collection and then coded and recoded, entered in SPSS, MS-Excel, Epi-info was used.
Measurement of Dental Caries, Oral Hygiene Status and Gum Bleeding
Dental Caries: Using the decayed missing and filled teeth (dmft) index for primary (4-5years) and early mixed (6-10years) and Decayed, Missing and Filled Teeth (DMFT) index for permanent dentitions. A tooth was considered decayed when there was frank carious cavities on any surface of the tooth. A tooth was as classified missing in the index if it was extracted due to caries.
Oral Hygiene Status
Using the Simplified Oral Hygiene Index (OHI-S) of Greene and Vermillon. The oral hygiene of each child was classified as ‘good’ when the OHI-S score was 0 to 0.06, ‘fair’ when it was 0.07 to 1.89 and ‘poor’ when it was 1.9 to 3. The criteria described by GREEN & VERMILLION, 1960 and 1964 were selected. Calculus was excluded. For the ages 4 to 6 years selected labial surfaces of the 54, 61, 82 and the lingual surface of 75. For the mixed dentition added the labial surface of 26 and the lingual surface of 46 [11]. Gingival bleeding: Gum bleeding was measured by slightly probing along with gingival sulcus. After probing it was resulted according to presence and absence of bleeding.
Ethical Issues
The approval letter for the conduction of research on specified topic was taken from the AIUB and Dhaka Dental Hospital. Informed consent was taken from each respondent, that was included objective of the study, time duration, privacy and confidentiality of information taken and information about participant can withdraw anytime.
Results
Socio-Demographic Factors
The purpose of the study was to find out practices and oral hygiene status among the children who were aged between 4 to 14 years. The present observation reveals that 40% of children were between 4-6 years of age, 24.35% between 7-8 years of age, 16.52% between 9 to 10 years and 19.13% between 11-14 years of age. Among the total study participants, there were 52.17% male respondents and 47.83% female respondents. In the present investigation, among 4 to 6 years children 21.74% was male and 18.26% was female, among 7 to 8 years children 12.17% was male and 12.17% was female, among 9 to 10 years children 10.43% was male and 6.09% was female and among 11 to 14 years children 7.83 was male and 11.3 was female (Figure 1).

Figure 1: Distribution of the respondents according to their age and gender.
Educational Level of the Children
In the present study, 26.09 percent were preschool going, 13.91 percent of respondents had education from play to class 1, 30.91 percent of respondents have education from class 2 to class 5 and 29.57 percent of respondents have education from class 6 to class 8 Table 1. Out of the 115 children 51.33% brushed their teeth once daily and 48.67% brushed their teeth twice daily (Figure 2).
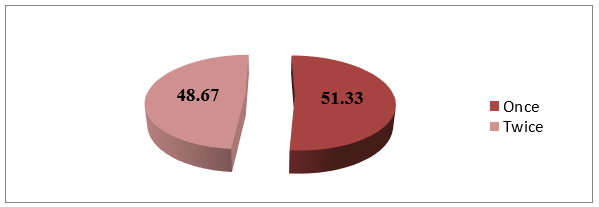
Figure 2: Habit of daily tooth brushing.
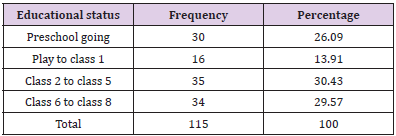
Table 1: Distribution of the children by their educational status.
Factors Related to Oral Hygiene Practices
It was observed that, 41.74% respondents brushed their teeth before breakfast, 6.09% brushed their teeth after breakfast, 1.74% brushed their teeth before meal at night, 1.74% brushed their teeth after meal at night, and 39.13% brushed their teeth before breakfast and after meal at night and 9.57% brushed their teeth after breakfast and after meal at night Table 2. Study shows that 98.26% respondents use toothbrush for brushed their teeth, 0% use Neem stick for brushed their teeth and 1.74% use finger for brushed their teeth (Figure 3). This study Table 3 reveals that 2.61% respondents changed their toothbrush after 1 to 2 months, 39.13% changed their toothbrush every 3 months, 24.35% changed their toothbrush every 4 months, 14.78% changed their toothbrush every 5 months, 15.65% changed their toothbrush every 6 months and 3.48% were lost their toothbrush within 1 month Table 3. Table 4 reveals that 0% respondents used mouthwash, 0% used floss, 0% used toothpick, 40% did simple gurgle after dinner at night and 60% used nothing Table 4.
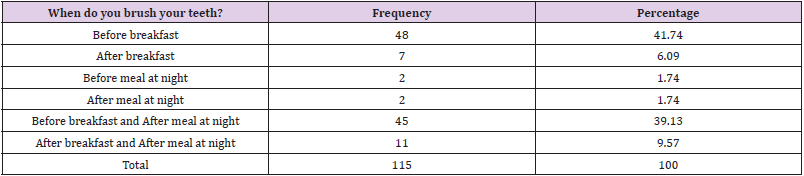
Table 2: Time schedule of tooth brushing.
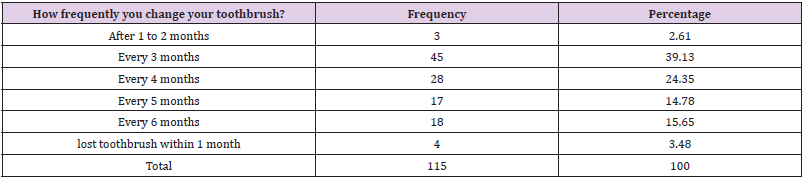
Table 3: Duration of toothbrush changing.

Table 4: Material used for clean teeth after dinner at night.
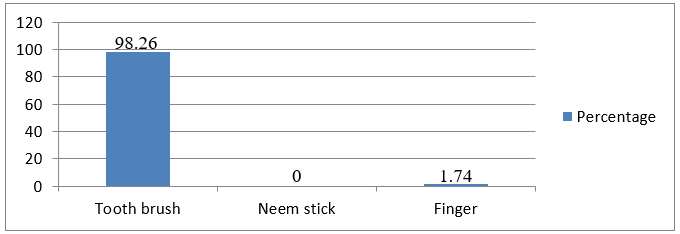
Figure 3: Tools used for cleaning teeth.
Factors Related to Visit to a Dentist
It was found that, 70.43% children visited dentist that day has also visited earlier and 29.57% visited for the first time. Study shows that out of the 81 children who visited dentist that day has also visited earlier 14.81% visited dentist regularly, 66.67% visited whenever there is a problem and 18.52% answered don’t know. It was observed that out of 115 children the oral hygiene status was good in 15.65%, oral hygiene status was fair in 37.39% and 46.96% had poor oral hygiene status Table 5. Study shows that out of 115 children, dental caries was present in 92.17% of them .Out of 115, children 46 were 4 to 6 years children and among 4 to 6 years children total decayed (d), Missing (m), and filled (f), Teeth (t) was 215 which indicated dmft index 4.67, 28 were 7 to 8 years children and among 7 to 8 years children total decayed (d), Missing (m), and filled (f), Teeth (t) was 151 which indicated dmft index 5.39, 19 were 9 to 10 years children and among 9 to 10 years children total decayed (d), Missing (m), and filled (f), Teeth (t) was 84 which indicated dmft index 4.42 and there were 22 children between 11 to 14 years of age and among them total Decayed (D), Missing (M), Filled (F), Teeth (T) was 63 which indicated DMFT index 2.86. the total mean dmft among age between 4 to 9 years was 4.84 and total mean DMFT was 2.86 Table 6.

Table 5: Distribution of the respondents according to oral hygiene status.
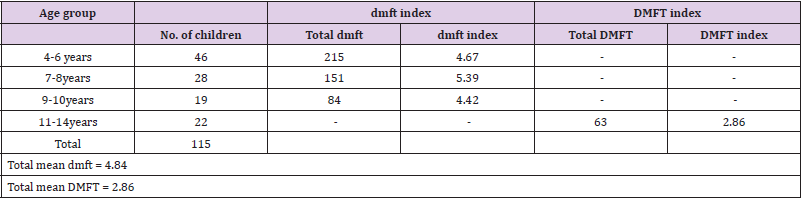
Table 6: Mean dmft/ DMFT of the study population according to age group.
In Figure 4, it was observed from the figure that among 4 to 6 years children the oral hygiene status was good in 11.31%, fair in 13.04%, good in 15.65%, among 7 to 8 years children the oral hygiene status was good in 1.8%, fair in 12.17% and poor in 10.43%, among 9 to 10 years children the oral hygiene status was good in 1.7%, fair in 6.09% and poor in 8.7% and among 11 to 14 years children the oral hygiene status was good in 0.87%, fair in 6.09% and poor in 12.7%. The study reveals that out of 60 male respondents 20.0% had good oral hygiene status, 40.0% had fair and 40.0% had poor oral hygiene status and out of 55 female respondents 10.9% had fair, 34.5% had and 54.5% had poor oral hygiene status (p>0.05). Therefore, there was no statistically significant relationship between gender and oral hygiene status Table 7. Study reveals that 57.6% respondents who brushed their teeth once daily had poor oral hygiene status and 35.7% respondents who brushed their teeth twice daily poor oral hygiene status (p<0.05) (Figures 5 & 6). So, the respondent who were brushed their teeth once daily had greater level of poor oral hygiene status than the respondent who were brushed their teeth twice daily. Therefore, there was statistically significant relationship between frequency of daily tooth brushing habit and oral hygiene status Table 8. Study reveals that 77.8% respondent who had poor oral hygiene status bad breath was present and bad breath was absent in 22.2% respondent who had poor oral hygiene status (p<0.05). So, the respondent who had bad breath oral hygiene status was poor. Therefore, there was statistically significant relationship between oral hygiene status and bad breath Table 9.
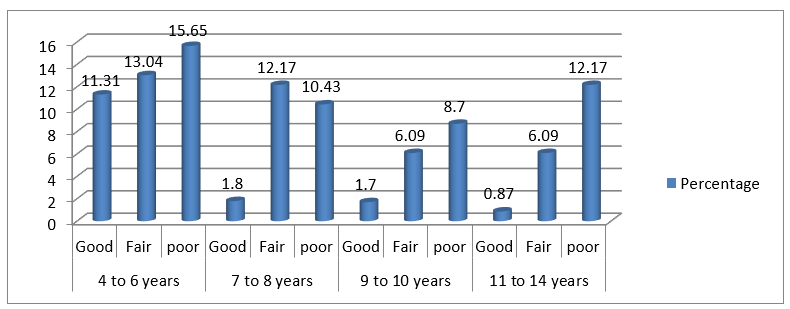
Figure 4: Distribution of the respondents according to their age group and oral hygiene status.
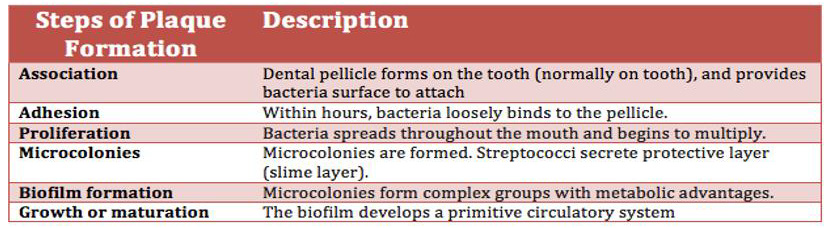
Figure 5.
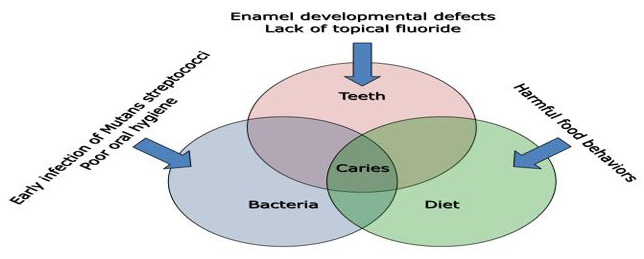
Figure 6.
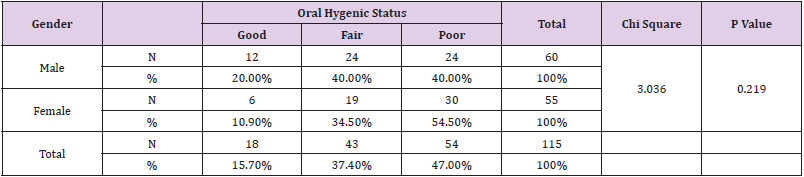
Table 7: Relationship between gender and oral hygiene status.
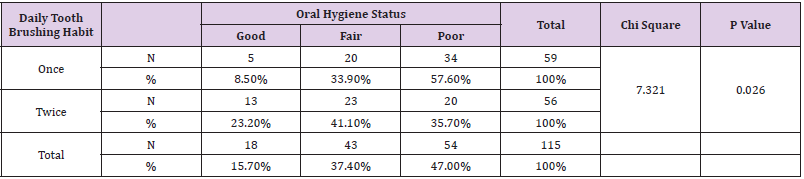
Table 8: Relationship between frequency of daily tooth brushing and oral hygiene status.
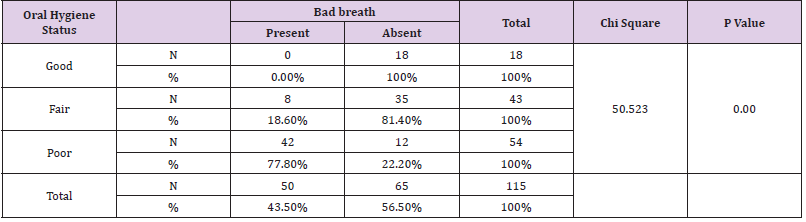
Table 9: Relationship between oral hygiene status and bad breath.
Discussion
Dental caries is a multi-factorial microbial infectious disease characterized by demineralization of inorganic and destruction of the organic substances of the tooth. Complications may include inflammation of the tissue around the tooth, tooth loss, and infection or abscess formation [12]. The cause of caries is acid from bacteria dissolving the hard tissues of the teeth (enamel, dentin and cementum). Simple sugars in food are these bacteria’s primary energy source and thus a diet high in simple sugar is a risk factor. If mineral breakdown is greater than build up from sources such as saliva, caries results. Gingivitisis a form of gum disease that happens when plaque, a naturally occurring sticky film containing bacteria, builds up on teeth and causes the inflammation of the surrounding gum tissue. Plaque produces toxins that irritate the gums [13]. The most common form of gingivitis, termed plaque-induced gingivitis is reversible with good oral hygiene; however, without treatment, gingivitis can progress to periodontitis, in which the inflammation of the gums results in tissue destruction and bone re-absorption around the teeth, ultimately lead to tooth loss [14]. Lack of awareness about the dental disease and proper treatment facilities are the main cause of poor dental condition [15,16]. Dental caries and periodontal disease are still the most important problems that are frequently seen and observed among children attending to the dental hospitals [17].
Factors related to oral hygiene practices: And it is evident in some study that most of the children brushed their teeth once daily and mainly brushed their teeth before breakfast [3,15]. According to American dental association the ideal tooth brushing time is 2 minutes and 2 times daily after breakfast and after meal. In the present study 98.26% respondents use toothbrush for brushed their teeth, 0% use neem stick for brushed their teeth and 1.74% use finger for brushed their teeth. 98.26% respondents use toothpaste for brushed their teeth, 1.74% use cinder for brushed their teeth and 0% use toothpowder for brushed their teeth. It was observed that most of the respondents didn’t use any tooth cleaning material after dinner at night only 40% respondent did simple gurgle at night after dinner.
Association
Lack of maintenance of proper oral hygiene practices are mainly responsible for poor oral hygiene status. In this study out of 115 children gingival bleeding was present in 41.74% and absent in 58.26%. Therefore, there was statistically significant relationship between oral hygiene status and parents’ total monthly income of the respondent. In India a study found that lower grade participants had poor oral hygiene status compared to higher grade participants [18]. Out of 60 male respondents, 20.0% had good oral hygiene status, 40.0% had fair and 40.0% had poor oral hygiene status and out of 55 female respondents 10.9% had fair, 34.5% had and 54.5% had poor oral hygiene status (p>0.05) [19- 22]. Therefore, there was no statistically significant relationship between gender and oral hygiene status. Respondents (57.6%) who brushed their teeth once daily had poor oral hygiene status and 35.7% respondents who brushed their teeth twice daily poor oral hygiene status (p<0.05). So, the respondent who were brushed their teeth once daily had greater level of poor oral hygiene status than the respondent who were brushed their teeth twice daily. Therefore, there was statistically significant relationship between frequency of daily tooth brushing habit and oral hygiene status [23-28]. Majority respondent (77.8%) who had poor oral hygiene status, had bad breath was present and bad breath was absent in 22.2% respondent who had poor oral hygiene status (p<0.05). So, the respondent who had bad breath oral hygiene status was poor. Therefore, there was statistically significant relationship between oral hygiene status and bad breath.
Conclusion
The findings have resulted from a cross sectional descriptive study done to assess the practices and oral hygiene status among 115 children aged 4 to 14 years attend to Dhaka Dental College and Hospital, Dhaka, Bangladesh. Bad breath was present in 43.48% children and was absent in 56.52% children out of 115 children. Study reveals that 77.8% respondent who had poor oral hygiene status bad breath was present and bad breath was absent in 22.2% respondent who had poor oral hygiene status. So, the respondent who had bad breath oral hygiene status was poor. Therefore, there was statistically significant relationship between oral hygiene status and bad breath. It was observed in this study that most of the children were fond of sugary and carbohydrate foods and drinks and took this kind of food almost every day and they also did not wash their mouth with water after taking any sugary and carbohydrates foods and drinks. In this study out of 115 children dental caries was present in 92.17% and absent in 7.83%. The survey revealed that in the age group 4 to 6 years the dmft index was 4.67, 7 to 8 years the dmft index was 5.39, 9 to 10 years the dmft index was 4.42 and among 11 to 14 years the DMFT index was 2.86. Sugary and carbohydrate foods are main reason of dental caries formation and did not clean mouth with water after taking any sweet and carbohydrate food increase dental caries formation.
Most of the children visited dentist second time and they visited whenever there is a pain or troubles with teeth or gums and for extraction of tooth. To maintain proper oral hygiene practices and oral hygiene status it is necessary to visit a dentist or dental hospital regularly. To maintaining good oral hygiene status simple preventive measures should be followed like proper brushing techniques and brushing the teeth twice daily and eating of less sticky food and avoidence of suger containing food as far as possible and rinsing of the mouth properly after taking sweet food and regular visit to a dentist and dental hospital is beneficial for children.
For more Articles on: https://biomedres01.blogspot.com/




No comments:
Post a Comment
Note: Only a member of this blog may post a comment.